
Heel Spur: Symptoms, Causes And Complete Treatment Guide
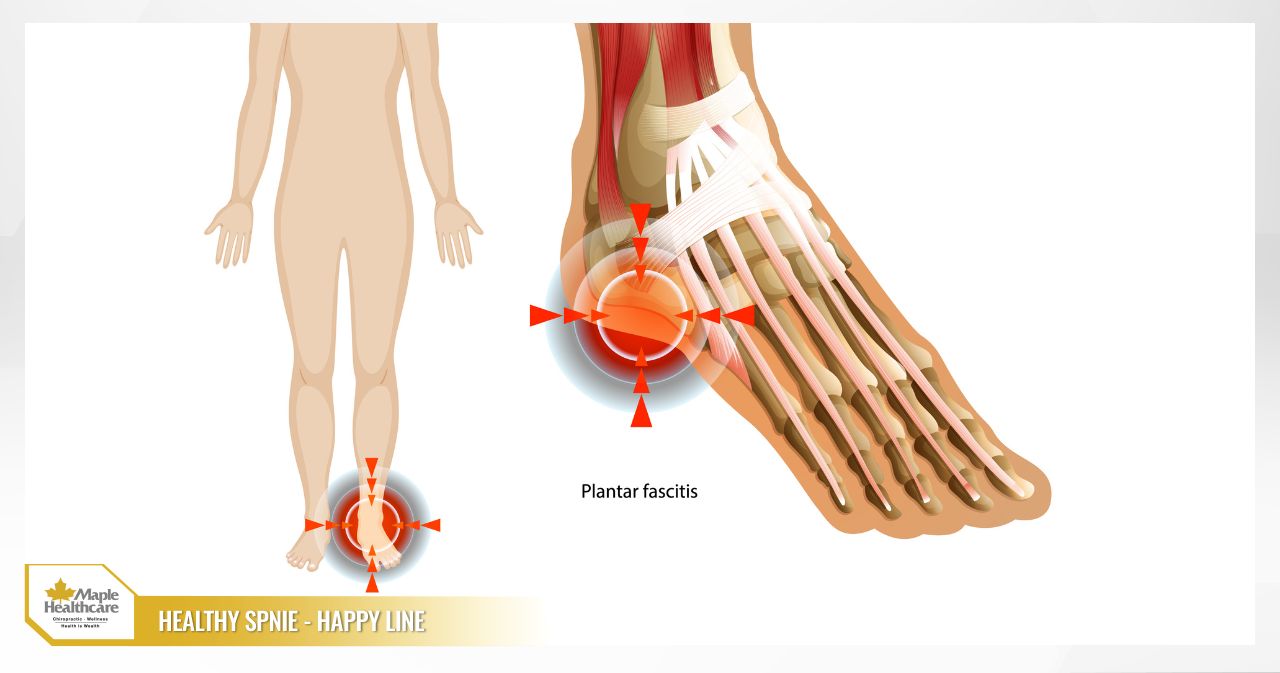
A heel spur is one of the most common causes of heel pain, turning those first steps out of bed each morning into a sharp, stabbing challenge. Many people believe the pain comes from a literal “bony spike” jabbing into soft tissue — but the reality is more nuanced. In most cases, the discomfort you feel is linked to inflammation or degeneration of a structure called the plantar fascia, rather than the bony growth visible on an X-ray. That characteristic sharp pain with your first few steps after waking up or after prolonged sitting occurs because the plantar fascia tightens overnight and is then suddenly stretched the moment you put weight on your foot.
Misunderstanding the nature of a heel spur can lead to ineffective treatment and prolonged discomfort. This article is designed as a comprehensive guide to help you distinguish the true source of your pain, recognise the symptoms early, and — most importantly — follow an evidence-based conservative treatment plan you can begin at home over 6–12 weeks. Maple Healthcare will also walk you through specific rehabilitation exercises, how to choose supportive footwear and insoles, and practical tips to prevent the pain from coming back. Throughout the article, terms such as “heel bone spur” and “calcaneal spur” are used interchangeably so you can more easily identify your condition.
What Is a Heel Spur — And How Is It Different from Plantar Fasciitis?
To manage your pain effectively, the most important first step is understanding what is actually causing it. Although often grouped under the umbrella term heel spur, there are two distinct concepts worth separating:
- Heel Spur (Calcaneal Spur): This is a small bony outgrowth (a calcium deposit) that forms on the underside of the heel bone (the calcaneus). It develops gradually over time, typically as the body’s response to repeated pulling and tension at the point where the plantar fascia attaches to the heel bone. In essence, the “spur” itself is the result of prolonged mechanical stress.
- Plantar Fasciitis: This refers to inflammation — or, more precisely in histological terms, degeneration — of the plantar fascia, a thick band of fibrous tissue that runs along the sole of the foot from the heel bone to the base of the toes. This structure acts like a bowstring supporting the arch of the foot and absorbing impact as you move. When it is overloaded, it sustains microscopic damage, resulting in pain and stiffness. This is the primary cause behind the vast majority of heel pain cases.

So what is the relationship between these two conditions, and where do they differ?
- The connection: The repeated pulling forces on the plantar fascia — the very forces that cause plantar fasciitis — are also what stimulate the body to form a bony spur. This is why both conditions are often found together on X-ray images.
- The key difference: The critical point here is that the bony spur itself is usually not what causes the pain. Research shows that many people have a heel spur visible on X-ray but experience no symptoms whatsoever. Conversely, many people with classic plantar fasciitis pain have no spur at all. The pain you feel comes primarily from the inflamed and damaged soft tissue — the plantar fascia — not from the spur pressing into anything.
This explains why your pain can be severe even when an X-ray looks “normal.” X-rays are excellent at evaluating bone, but they are poorly suited for detecting damage in soft tissues such as tendons and ligaments.
Heel Spur Symptoms and How to Recognise Them Early
The symptoms associated with a heel spur and plantar fasciitis tend to follow a recognisable pattern. Here are the key signs to watch for:
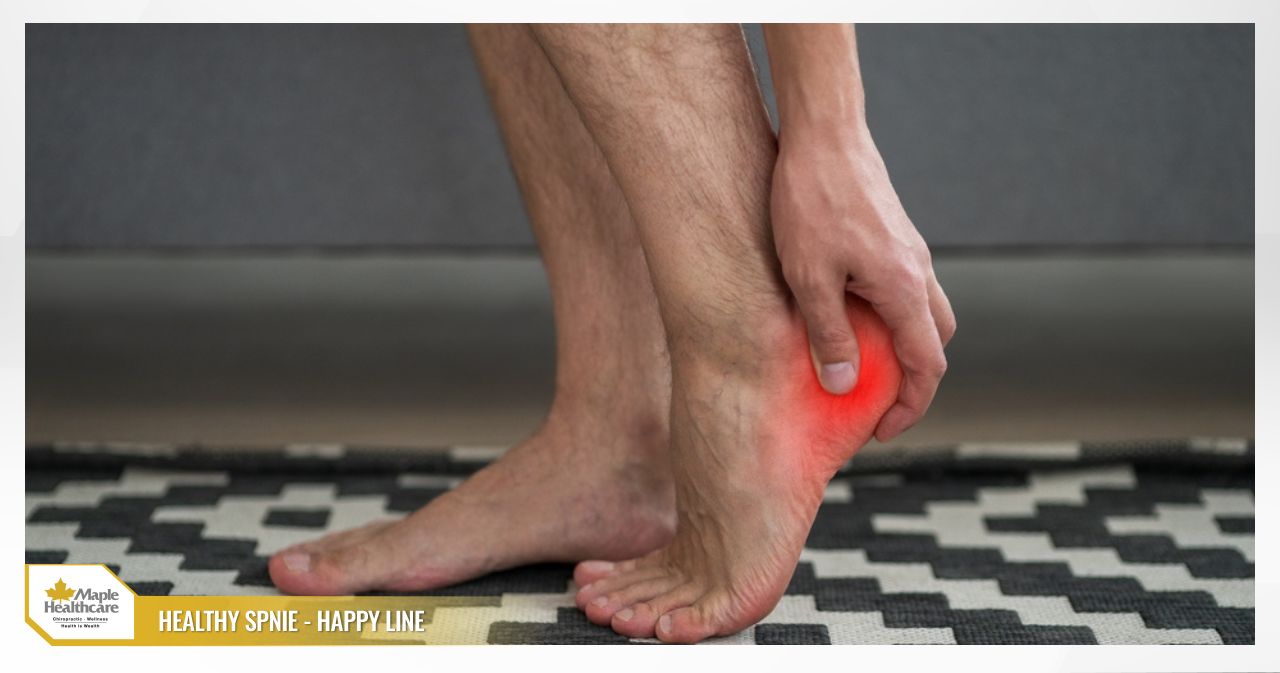
- Characteristic pain pattern: The pain is typically described as sharp, stabbing, or like stepping on a tack, felt on the underside of the heel. It is usually most intense at the inner edge of the heel, where the plantar fascia attaches to the heel bone. Pressing firmly on this spot will often reproduce the pain.
- When pain is worst: The most telling symptom is pain during your first steps in the morning after getting out of bed, or after sitting for a prolonged period and then standing up. After walking for a few minutes, the pain may ease as the plantar fascia “warms up” and loosens. However, it is likely to return and worsen towards the end of the day if you spend long periods on your feet.
- Factors that aggravate the pain:
- Standing in one position for a long time.
- Walking or running long distances.
- Walking barefoot on hard surfaces such as tile or concrete floors.
- Carrying or lifting heavy loads.
- Associated signs:
- Stiffness around the heel, particularly in the morning.
- A feeling of tightness or aching in the calf muscles.
- Reduced ankle dorsiflexion range of motion (difficulty pulling your toes up towards your shin).
You can try a simple self-check at home using the Windlass test: Sit in a chair and use one hand to bend your big toe and the other toes back towards your shin. If this movement creates a stretch along the sole of your foot and reproduces your familiar heel pain, there is a good chance your plantar fascia is involved.
Causes and Risk Factors for Heel Spurs
Heel spurs and plantar fasciitis do not arise without reason. They are the result of repeated stress and overload on the plantar fascia structure. The leading causes and risk factors include:
- Primary mechanism: Repetitive loading of the plantar fascia and its attachment point on the heel bone. This commonly occurs when you suddenly increase the volume, intensity, or frequency of weight-bearing activity — such as walking or running — without giving your body adequate time to adapt.
- Biomechanical abnormalities:
- Flat feet (Pes Planus): When the arch collapses, the plantar fascia is placed under excessive tension with every step.
- High-arched feet (Pes Cavus): A rigid foot with poor shock absorption places greater pressure on the heel and forefoot.
- External factors:
- Unsuitable footwear: Shoes with very thin or overly soft soles, insufficient arch support, or uneven wear can alter your gait mechanics and increase load on the heel.
- Prolonged standing or walking on hard floors: Tile and concrete surfaces offer no shock absorption, forcing your foot and heel to bear the full impact of each step.
- Individual factors:
- Excess body weight: Every additional kilogram of body weight places significantly greater force on the heel with each step or stride.
- Occupation: Jobs that require prolonged standing — such as teaching, factory work, or retail — carry a higher risk.
- Age: The condition is most common in middle-aged adults (40–60), as the plantar fascia gradually loses elasticity and the protective fat pad under the heel thins over time.
- Runners: Particularly those who increase their mileage or pace too quickly.
- Tight calf muscles: Tightness in the gastrocnemius or soleus muscles limits ankle range of motion, which indirectly increases the pulling force on the plantar fascia.

Diagnosing a Heel Spur
An accurate diagnosis is an essential step towards finding the right treatment approach.
Safe Self-Assessment at Home
- Locate the tender point: Press your thumb firmly into the underside of your heel, particularly the inner portion near the arch. If you find a specific, sharply tender spot, this is an important indicator.
- Perform the Windlass test: As described above, bend your toes back towards your shin and note whether this reproduces your usual heel pain.
Clinical Assessment at a Healthcare Facility
- Medical history: Your clinician will ask detailed questions about the nature of your pain, when it is at its worst (particularly morning pain), activities that aggravate or relieve it, the type of footwear you typically wear, and any recent changes in your activity habits.
- Physical examination: The clinician will palpate the heel to precisely identify the painful point, assess your foot arch structure, and test ankle dorsiflexion range of motion. A more specific test called the Silfverskiöld test may be performed to distinguish between tightness of the gastrocnemius versus the soleus muscle.
- Investigations:
- X-ray: May be ordered to check for the presence of a heel bone spur or to rule out other causes of heel pain such as a stress fracture. However, it is important to remember that the presence or absence of a spur does not determine the source of your pain.
- Ultrasound: A very useful tool for directly evaluating soft tissue. Ultrasound can reveal whether the plantar fascia is thickened (a sign of chronic degeneration), whether there is surrounding oedema, and can help rule out a partial tear of the plantar fascia. It is typically used when symptoms are persistent or atypical.
Differential Diagnosis
It is important to rule out other conditions that can also cause heel pain, such as:
- Achilles tendinopathy (pain at the back of the heel)
- Tarsal tunnel syndrome (pain accompanied by numbness, burning, or nerve-type symptoms)
- Calcaneal stress fracture (pain that worsens when the sides of the heel bone are squeezed)
- Gout or other inflammatory arthritis conditions
- Infection (rare; usually accompanied by redness, warmth, swelling, and fever)
You should seek medical attention promptly if you experience any of the following warning signs: sudden, severe pain following a trauma (a fall or jump), visible deformity of the heel, significant swelling, bruising, warmth, redness accompanied by fever, widespread numbness or weakness, or an inability to bear weight on the affected foot.
A Home Treatment Plan for Heel Spurs (6–12 Weeks)
The encouraging news is that more than 90% of heel pain cases related to plantar fasciitis can improve meaningfully with consistent conservative management over several weeks to a few months. Here is what you can do at home:
- Relative rest: This is the most important principle. Reduce or temporarily pause activities that cause significant pain, such as running, jumping, or long-distance walking. You can maintain fitness through low-impact alternatives like swimming or cycling. “Relative rest” does not mean complete inactivity.
- Ice therapy: Roll a bag of ice or a frozen water bottle under the sole of your foot for 10–15 minutes. Do this 2–3 times per day, particularly after activity or when pain flares up. Cold helps reduce inflammation and provides meaningful pain relief.
- Over-the-counter pain relief: Non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen or naproxen may help manage pain and inflammation in the short term. However, use them with caution if you have a history of stomach, kidney, or cardiovascular conditions, or if you are on blood-thinning medication. Consult a pharmacist or doctor before use. Topical NSAID gels applied directly to the skin are a safer option to minimise systemic side effects.
- Self-care techniques:
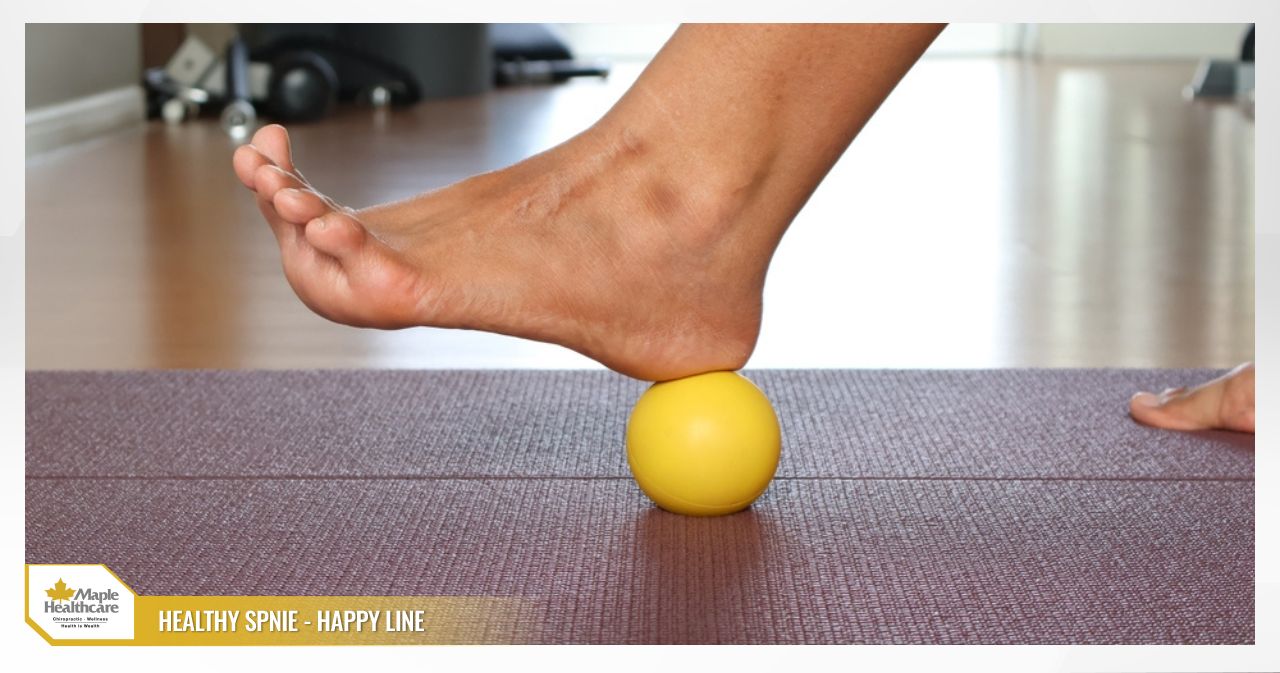
- Ball rolling: Use a tennis ball or a dedicated massage ball to gently roll under the sole of your foot for 5–10 minutes daily. This massages the plantar fascia and helps release built-up tension.
- Supportive taping: The Low-Dye taping technique can help support the arch and significantly reduce load on the plantar fascia during the acute pain phase.
- Ball rolling: Use a tennis ball or a dedicated massage ball to gently roll under the sole of your foot for 5–10 minutes daily. This massages the plantar fascia and helps release built-up tension.
- Monitoring your pain levels: Rate your pain on a scale of 0 (no pain) to 10 (worst imaginable). Apply the “no more than 2 points” rule: during and within 24 hours of performing any activity or exercise, your pain should not increase by more than 2 points above your baseline. If it does, reduce the intensity or volume of that activity.
Effective Exercises for Heel Spurs
Exercise is the foundation of recovery. The goal is to improve flexibility and build strength in the structures that support your foot.
Stretching Exercises (Perform Daily)
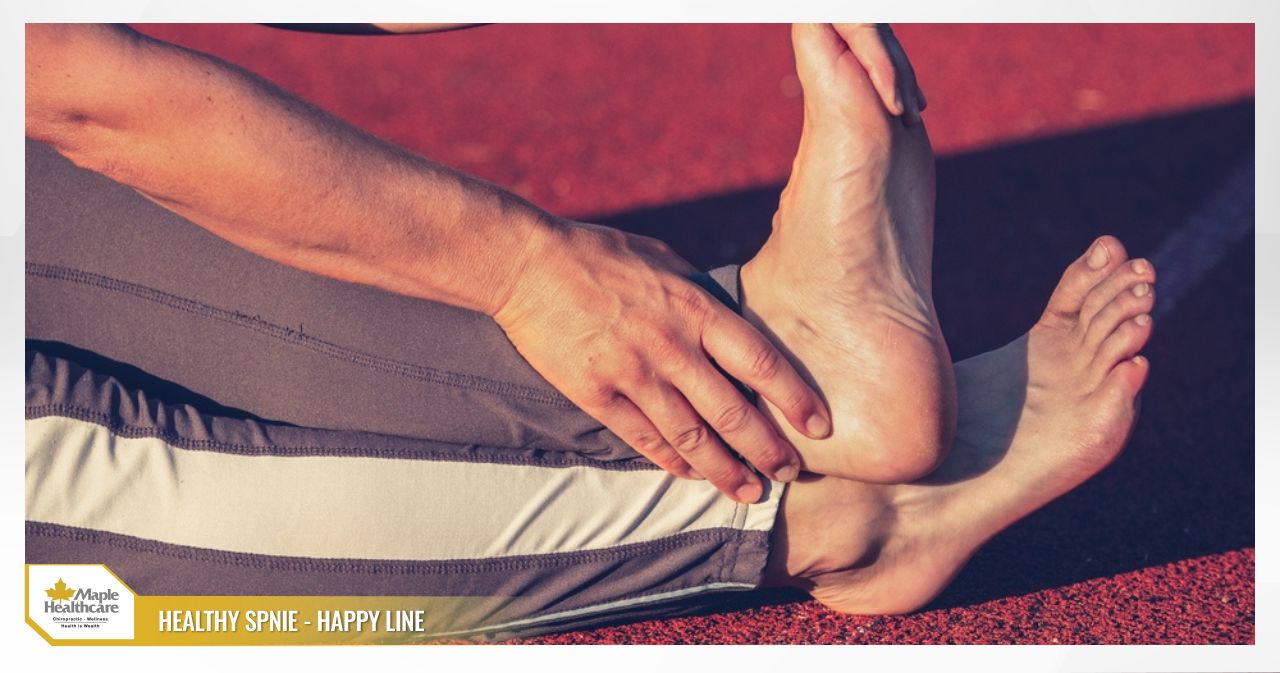
Plantar Fascia Stretch
- How to do it: Sit in a chair and cross your affected foot over the opposite thigh. Using your hand, gently pull your toes (especially the big toe) back towards your shin until you feel a stretch along the arch of your foot.
- Duration: Hold for 30 seconds, repeat 3–5 times per foot.
- Tip: Perform 2–3 times per day. It is especially helpful to do this before placing your feet on the floor in the morning to ease that painful “first step” sensation.
Gastrocnemius Calf Stretch
- How to do it: Stand facing a wall with both hands placed on it for support. Step your affected leg back, keeping the back knee straight and the heel flat on the floor. Slowly lean forward until you feel a stretch in the upper calf of the back leg.
- Duration: Hold for 30–45 seconds, repeat 3–5 times.
Soleus Stretch
- How to do it: Use the same position as above, but this time slightly bend the knee of the back leg. You should feel the stretch shift to the lower part of the calf.
- Duration: Hold for 30–45 seconds, repeat 3–5 times.
Strengthening Exercises (Perform Every Other Day)
Eccentric Calf Raises (Slow Heel Drops)
- How to do it: Stand on the balls of both feet on a step. Rise up on both heels, then transfer your weight to the affected foot only and slowly lower your heel down below the level of the step over 3–5 seconds.
- Frequency: Begin with 3 sets of 10–15 repetitions, 1–2 times per day. You can gradually increase difficulty by wearing a light backpack. Avoid allowing pain to increase significantly or persist after the session.
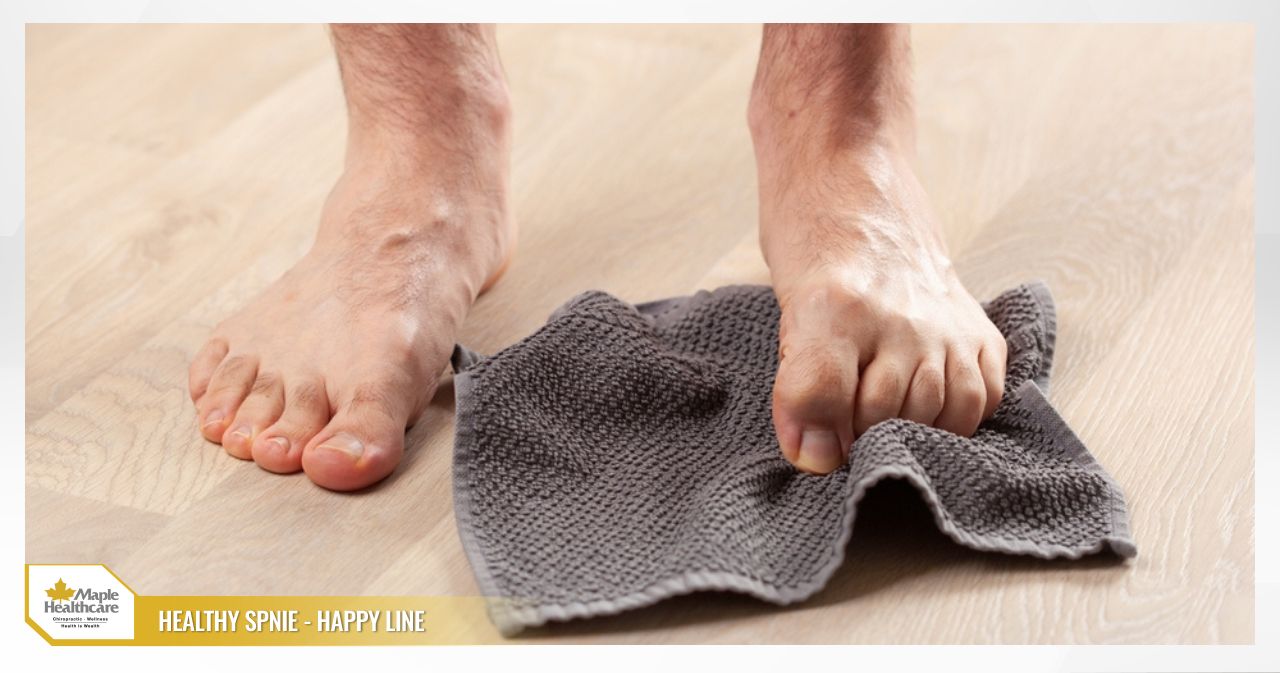
Towel Scrunches/Curls
- How to do it: Sit in a chair with a small towel laid flat on the floor. Use the toes of your affected foot to scrunch and pull the towel towards you.
- Frequency: 3 sets of 10–15 repetitions.
Short Foot Exercise
- How to do it: Sit in a chair with your foot flat on the floor. Gently contract the muscles in the sole of your foot to draw the ball of your foot towards your heel, creating a small arch — without curling your toes.
- Duration: Hold for 5–10 seconds, repeat 10–15 times. This exercise activates and strengthens the intrinsic muscles of the foot.
Sample Weekly Exercise Schedule
- Week 1: Prioritise stretching exercises 2–3 times per day. Add ball rolling. You may begin eccentric heel drops 3 times per week at a low intensity (no added weight).
- Weeks 2–3: If pain does not increase, continue stretching and gradually progress eccentric heel drops to 4–5 times per week. Add arch activation and towel curl exercises 3 times per week.
- Golden rule: Do not increase training volume (duration, repetitions, or load) by more than 10–20% per week. Always listen to your body and scale back if pain increases noticeably.
Choosing the Right Footwear, Insoles, and Supportive Devices
Selecting the right supportive equipment can make a meaningful difference in reducing the load on your heel.
- Shoes: Look for footwear with the following features:
- A firm heel counter: This securely cups the heel and prevents it from rolling inwards or outwards.
- Good arch support: Helps lift the arch and reduce strain on the plantar fascia.
- Moderate cushioning: Not too hard, but not excessively soft either. Ultra-soft shoes may feel comfortable initially but do not provide sufficient stability.
- Avoid completely flat, zero-drop shoes during the acute pain phase.
- Most importantly: replace your shoes when they are worn out, especially if the heel area shows uneven wear.
- Insoles and Heel Cups:
- Silicone heel cups can provide cushioning and absorb direct impact on the tender spot.
- Arch-support insoles (either off-the-shelf or custom-made) help redistribute pressure across the entire foot, reducing the burden on the plantar fascia. You can trial an over-the-counter option for 1–2 weeks to gauge effectiveness.
- Night Splints: For those who experience significant morning pain, a night splint can be a very helpful addition. This device holds the ankle at a 90-degree angle (or in slight dorsiflexion) while you sleep, preventing the plantar fascia and Achilles tendon from contracting overnight.
A common mistake: Many people focus solely on switching to ultra-soft shoes while overlooking the other core elements of recovery — such as exercise, load management, and addressing underlying biomechanical factors. Footwear is just one piece of the overall picture.
Medical Treatment When Home Remedies Are Not Enough
If self-care measures at home have not provided adequate relief after several months, it is worth seeking specialist support. Treatment options may include:
- Physiotherapy: This is the preferred first-line option. A physiotherapist will design a personalised exercise programme covering both stretching and strengthening. They may also apply manual therapy techniques to work on the plantar fascia and calf soft tissue, and provide detailed guidance on specialist taping methods.
- Extracorporeal Shockwave Therapy (ESWT): This technique delivers high-energy sound waves to the painful area of the heel to stimulate the body’s natural healing processes. ESWT is typically considered for chronic heel spur and plantar fasciitis cases (pain lasting more than six months) that have not responded to other conservative measures. A typical course involves 3–6 sessions, spaced approximately one week apart.
- Corticosteroid Injections: Injecting a strong anti-inflammatory medication into the heel can provide rapid short-term pain relief. However, this comes with important caveats. Repeated injections carry an increased risk of plantar fascia rupture and atrophy of the protective fat pad under the heel, which can worsen the problem over time. This option is therefore used with increasing caution and is not considered a first-line treatment.
- Platelet-Rich Plasma (PRP) Injections / Prolotherapy: These approaches involve injecting biologically active substances into the damaged tissue to support the repair process. Research evidence is growing but remains mixed, and these are not yet considered standard-of-care treatments.
- Surgery: Surgical intervention is rarely needed. It is only considered after all conservative treatment options have been exhausted over at least 6–12 months. Procedures may involve partially releasing the plantar fascia to relieve tension. Post-operative rehabilitation is an essential part of recovery and requires close professional guidance.
For cases that benefit from conservative care, clinicians at Maple Healthcare in Ho Chi Minh City can develop an integrated, personalised programme combining chiropractic care, physiotherapy, and rehabilitation — with the aim of addressing the underlying mechanical causes of pain, improving functional movement, and supporting long-term recovery.
When to Seek Medical Attention Promptly
While most cases of heel pain are benign, you should seek medical attention without delay if you experience any of the following red flag symptoms:
- Sudden, severe pain following a trauma such as a fall or jump.
- Visible deformity, significant swelling, or bruising of the heel.
- Complete inability to stand or bear weight on the affected foot.
- Signs of serious infection in the heel area: redness, a burning sensation to the touch, and accompanying fever.
- Spreading pain accompanied by numbness, tingling, burning, or muscle weakness in the foot or lower leg (possible signs of nerve compression).
- No improvement after 6–12 weeks of appropriate self-management.
- You have an underlying health condition such as diabetes or systemic inflammatory arthritis (e.g., rheumatoid arthritis), as the potential causes and complication risks may be more complex.
Preventing Heel Spurs from Coming Back
Once your pain has settled, maintaining good habits is the key to keeping a heel spur from recurring:
- Increase load gradually: Always follow the “10% rule.” Do not increase your weekly running or walking distance or intensity by more than 10% at a time. Include recovery days between high-intensity training sessions.
- Manage your body weight: Maintaining a healthy weight is one of the most effective ways to reduce the daily strain placed on your feet.
- Keep up your stretching routine: Make plantar fascia and calf stretches a regular part of your daily routine — much like brushing your teeth. Perform them in the morning and after physical activity.
- Check your footwear regularly: Do not hold onto worn-out shoes. Replace both shoes and insoles on a regular basis. If your job requires prolonged standing, take short micro-breaks throughout the day to sit down or walk around gently.
- Cross-train: Incorporating low-impact activities such as swimming and cycling into your exercise routine gives your musculoskeletal system time to rest and supports well-rounded fitness.

Common Myths and Misconceptions About Heel Spurs
- Myth: “My pain is caused by the bone spur itself. I need surgery to remove it before I can get better.”
Reality: As explained above, the pain is primarily driven by plantar fascia inflammation. The vast majority of people improve well with conservative management, without any intervention directed at the bony spur. - Myth: “If I just rest completely and stay off my feet, it will go away on its own.”
Reality: Complete rest may temporarily reduce pain, but it also leads to muscle weakness and joint stiffness, making it more likely that symptoms will return once you resume activity. “Smart load reduction” combined with targeted exercise is the more effective strategy. - Myth: “I just need to switch to softer shoes and it will fix itself.”
Reality: Ultra-soft shoes lack the support and stability your foot needs. Good footwear requires the right balance of cushioning, arch support, and heel stability.
FAQ: Frequently Asked Questions About Heel Spurs
How long does a heel spur take to heal, and can it resolve on its own?
Answer: With consistent conservative management — including load reduction, targeted exercise, and appropriate footwear — many people begin to notice improvement within a few weeks, and symptoms may resolve significantly within 6–12 months. The condition is unlikely to improve on its own if the underlying risk factors are not addressed.
Is heat or ice better for a heel spur?
Answer: Ice is generally the better choice during the acute pain phase and after activity, as it helps reduce inflammation and ease discomfort. Heat may help relax the muscles before stretching in some people, but should be avoided when the heel is actively swollen or painful.
Can I run if I have a heel spur?
Answer: If running noticeably worsens your pain, it is advisable to pause or significantly reduce the intensity and frequency of your runs. Once your pain is well managed, you can return to running gradually, following the 10% loading rule strictly.
When is an X-ray or ultrasound needed to diagnose a heel spur?
Answer: Your clinician may recommend imaging if your symptoms are atypical, do not respond to initial treatment, or if other causes such as a stress fracture or joint disease need to be ruled out.
Which insoles are best? Do I need custom orthotics?
Answer: Many people do well with off-the-shelf arch-support insoles. However, if you have a more complex foot structure (very flat or very high-arched) or persistent symptoms, a professional assessment and a custom-made orthotic may provide better results.
How is a heel spur different from Achilles tendinopathy?
Answer: A heel spur and plantar fasciitis cause pain on the underside of the heel. Achilles tendinopathy, on the other hand, causes pain at the back of the heel, at the point where the Achilles tendon inserts into the heel bone.
Should I get a corticosteroid injection for a heel spur?
Answer: This option warrants careful consideration. While it can provide rapid short-term relief, there is a real risk of weakening the plantar fascia (potentially leading to rupture) and causing atrophy of the heel’s protective fat pad. It is not considered a first-line treatment option.
Can diet help with heel spur recovery?
Answer: A balanced, anti-inflammatory diet that supports healthy weight management can contribute to the body’s overall recovery. However, no specific food can substitute for the core mechanical treatments — exercise and appropriate footwear adjustments — that are central to managing this condition.
Related articles:
Foot and Heel Pain
Ankle Ligament Tear: Causes and Treatment Explained
Knee Osteoarthritis: What It Is and Effective Supportive Care.
Contact for consultation
MAPLE INTERNATIONAL CO., LTD
Phone: 0705 100 100
Tax code: 0311948301
Date Range: 21 - 08 - 2012
Issued: Department of Planning and Investment of Ho Chi Minh City
Healthcare Group Members

Contact Us
COPYRIGHT

![]()


