Knee Osteoarthritis: What It Is and Effective Supportive Care.
Do you find yourself troubled by aching pain, stiffness, or discomfort in your knees during movement or when the weather changes? These may be the first signs of knee osteoarthritis. This is a chronic condition characterised by the gradual wearing down of the articular cartilage and a decline in the quality of joint fluid, causing the bone ends to rub against each other and resulting in pain and stiffness. Common in older adults and athletes alike, knee osteoarthritis can significantly affect your mobility and quality of life.
Understanding knee osteoarthritis not only helps you recognise symptoms early, but is also the key to choosing the right treatment approach, building a safe exercise plan, and slowing the progression of the condition. This article serves as a comprehensive guide, walking you through each step of managing the condition — including a detailed 4–8 week practical plan.
Overview of Knee Osteoarthritis
Knee osteoarthritis is a chronic musculoskeletal condition that progresses slowly and is characterised by comprehensive damage to the knee joint. This process involves:
- Cartilage wear: The smooth cartilage layer covering the ends of the bones gradually thins, cracks, and wears away.
- Subchondral bone changes: The bone beneath the cartilage becomes denser and bone spurs (osteophytes) form at the edges of the joint.
- Reduced joint fluid quality: The amount of lubricating fluid within the joint decreases and its viscosity diminishes, leading to increased friction.
- Synovial membrane inflammation: The inner lining of the joint becomes mildly inflamed, causing swelling and pain.
All of these changes lead to a narrowing of the joint space, causing pain, restricted movement, and potentially joint deformity over time.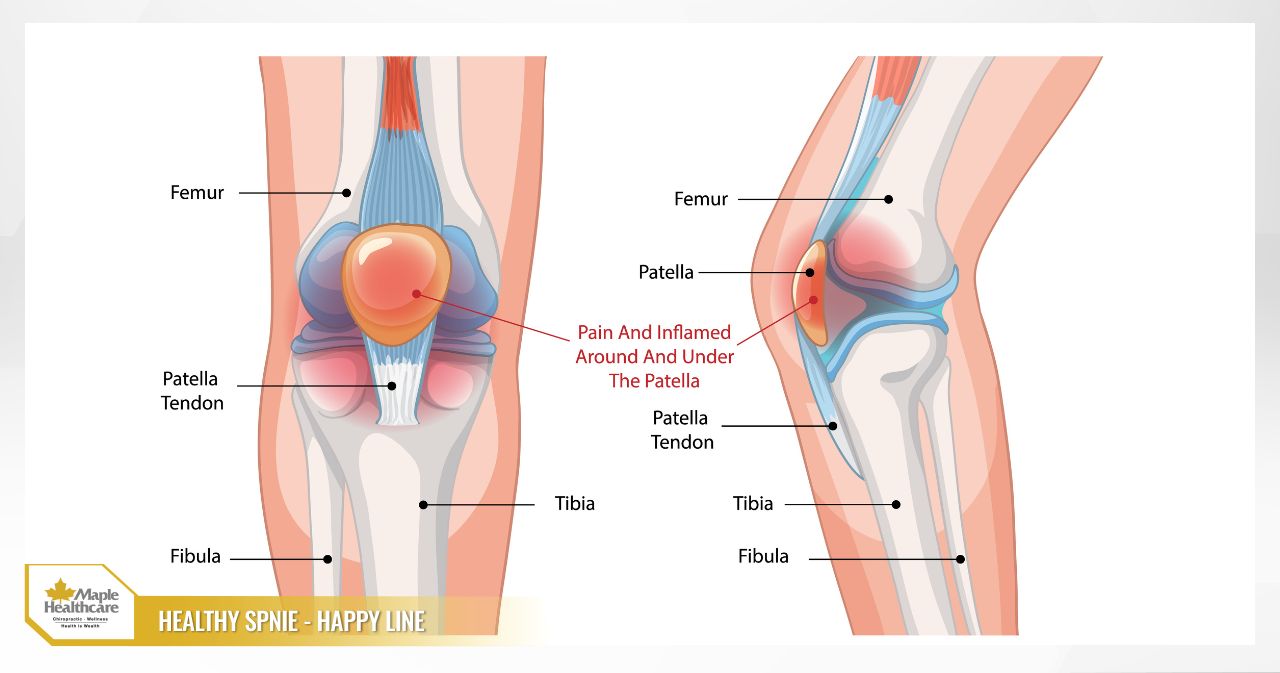
How Knee Osteoarthritis Differs from Other Conditions
- Rheumatoid arthritis: An autoimmune disease that typically affects multiple joints symmetrically (both knees). Morning stiffness lasting more than 60 minutes is a hallmark symptom.
- Gout: Causes acute episodes of joint inflammation with swelling, warmth, redness, and intense pain, typically starting in the big toe joint due to the deposition of urate crystals.
- Meniscal injury: Usually caused by a twisting or pivoting injury to the knee, producing mechanical-type pain, and sometimes accompanied by a sensation of catching or locking in the joint.
Who Is at Higher Risk?
- Older adults: Risk increases noticeably after the age of 60.
- Women: Particularly those who have gone through menopause.
- Overweight or obese individuals: Excess body weight places significant additional load on the knee joints, accelerating the degenerative process.
- Family history: Genetic factors also play a contributing role.
- Previous injuries: A history of fractures, ligament tears, or knee surgery.
- Occupation: Jobs requiring prolonged standing, heavy lifting, or repetitive knee bending.

Signs and Symptoms of Knee Osteoarthritis
The symptoms of this condition typically develop gradually. Recognising them early will help you seek timely support.
Typical Symptoms
- Knee pain: This is the primary symptom. The pain is “mechanical” in nature — meaning it worsens with activity (walking, climbing stairs, sitting down or standing up) and eases with rest. Pain often feels worse towards the end of the day.
- Morning stiffness: A feeling of stiffness and difficulty moving the knee joint after waking up, although this typically resolves within 30 minutes.
- Clicking or grinding sensations in the joint: You may hear or feel a crunching or cracking sound when bending or straightening the knee.
- Joint swelling: The knee may become mildly swollen or develop recurring fluid build-up, particularly after periods of increased activity.
- Reduced range of motion: Difficulty fully bending or straightening the knee.
- Muscle weakness: The quadriceps muscle (at the front of the thigh) may weaken, making the leg feel unsteady.
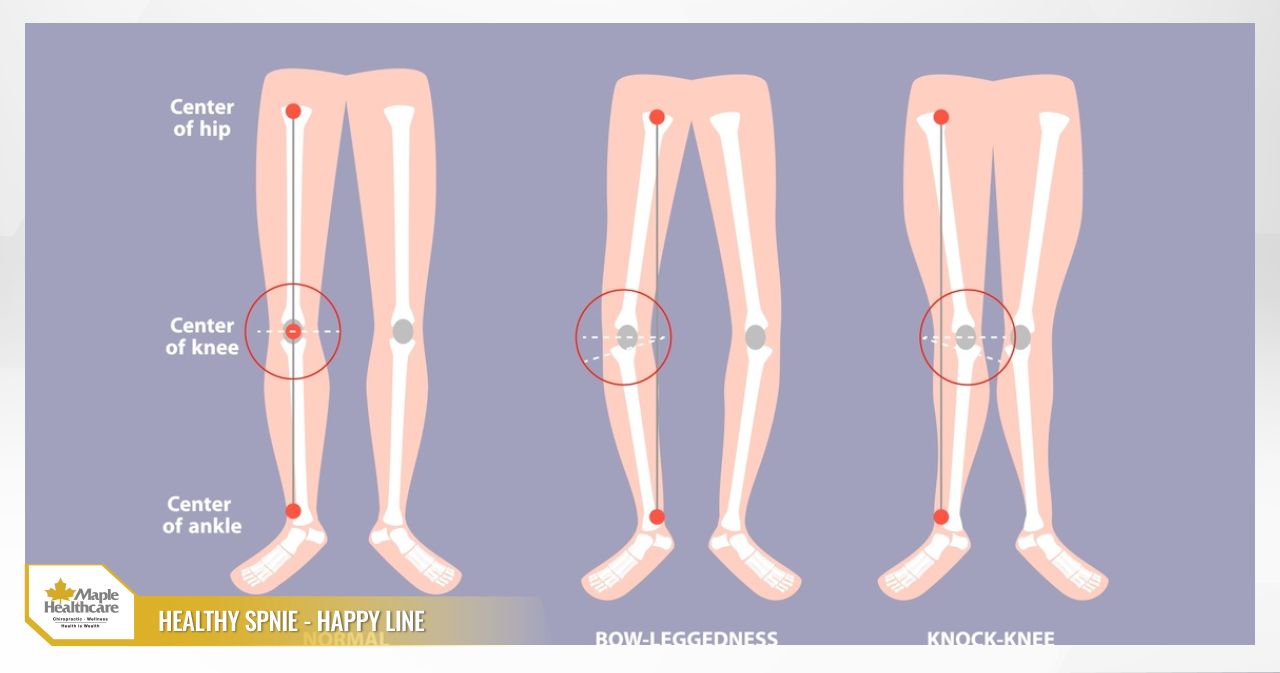
- Joint deformity: In later stages, the knee joint may become deformed, bowing inward (bow-legged / varus deformity) or outward (knock-kneed / valgus deformity).

Factors That Can Trigger a Flare-Up
- Prolonged squatting or kneeling.
- Climbing many flights of stairs.
- Deep knee bending.
- Changes in weather, especially when it turns cold or humid.
Causes and Risk Factors of Knee Osteoarthritis
Knee osteoarthritis does not arise from a single cause — rather, it results from a combination of several contributing factors:
- Age: This is the primary risk factor. Over time, the ability of cartilage cells to repair and regenerate themselves diminishes, making the joint cartilage increasingly vulnerable to damage and wear.
- Being overweight or obese: Each additional kilogram of body weight places several times more force on the knee joints during everyday activities. Obesity not only increases mechanical load but also promotes systemic inflammation, which can worsen the condition.
- Previous injuries and surgery: Prior injuries such as meniscal tears, anterior cruciate ligament (ACL) ruptures, or fractures around the knee joint alter the mechanics of the joint and increase the risk of osteoarthritis later in life.
- Genetics and bone structure: Some individuals have a genetic predisposition to weaker cartilage, or an abnormal lower limb alignment (bow-legs or knock-knees) that places disproportionate stress on a specific area of the knee joint.
- Occupational and sporting activities: Jobs or sports that require repetitive knee bending, twisting, or load-bearing can increase risk. Conversely, a very sedentary lifestyle can weaken the surrounding muscles and cause joint stiffness, which is also harmful to the knee.
- Other medical conditions: Rheumatoid arthritis, gout, or metabolic disorders can damage the joint and lead to secondary osteoarthritis.
How Knee Osteoarthritis Is Diagnosed
To reach an accurate diagnosis, your clinician will use a combination of approaches. At Maple Healthcare in Ho Chi Minh City, we always begin by taking the time to listen carefully to your concerns.
- Clinical examination: Your clinician will ask about your medical history, the symptoms you are experiencing, and what makes the pain better or worse. They will then examine your knee to assess range of motion, identify points of tenderness, evaluate joint stability, and observe your leg alignment.
- Imaging studies:
- X-ray: This is the most fundamental and important diagnostic tool. X-rays can reveal characteristic signs such as joint space narrowing, bone spurs, and subchondral bone sclerosis. Based on these images, your clinician can grade the severity of the condition using the Kellgren-Lawrence scale.
- Ultrasound or MRI: These are typically ordered when your clinician needs to further assess soft tissue structures such as the menisci and ligaments, or when the diagnosis remains unclear.
- Blood tests: These are primarily carried out to rule out other inflammatory joint conditions such as rheumatoid arthritis or gout.
An accurate assessment of disease stage is essential in determining the most appropriate treatment strategy for you.
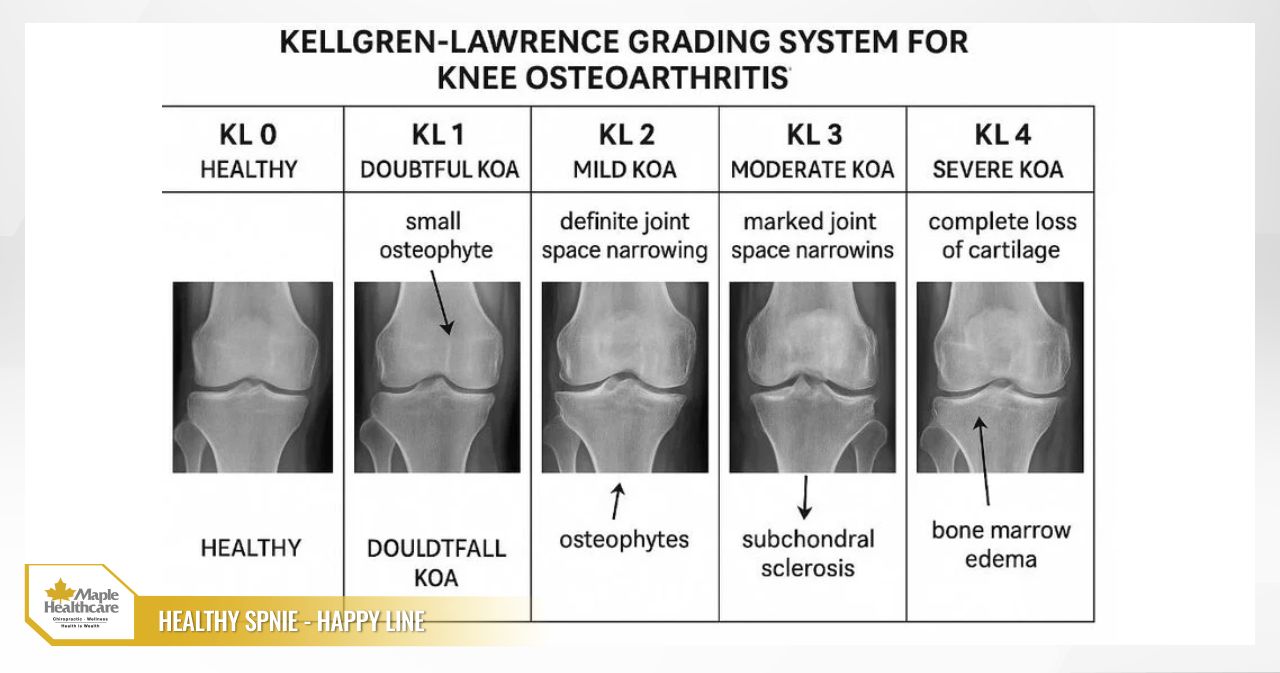
Disease Severity and Progression — The Kellgren-Lawrence Grading Scale
The Kellgren-Lawrence (K-L) grading system, based on X-ray findings, is a widely used method for assessing the severity of knee osteoarthritis and guiding treatment decisions.
- Grade 1 (Doubtful): Possible very small bone spurs; joint space appears normal. This stage often produces no clear symptoms.
- Grade 2 (Mild): More clearly visible bone spurs; joint space still appears normal. You may begin to notice mild pain after prolonged activity.
- Grade 3 (Moderate): Definite bone spurs, moderate joint space narrowing, and possible subchondral bone sclerosis. Pain and stiffness become more frequent.
- Grade 4 (Severe): Marked joint space narrowing or fusion, large bone spurs, and deformity of the subchondral bone. Significant pain, severely restricted movement, and a major impact on quality of life.
Complications and Impact on Quality of Life
If not properly managed, knee osteoarthritis can lead to a number of significant consequences:
- Serious functional limitations: Difficulty with daily activities such as walking, climbing stairs, sitting and standing, and even basic self-care.
- Muscle wasting and joint instability: Pain and reduced activity cause the muscles surrounding the knee — particularly the quadriceps — to weaken and atrophy. This makes the knee joint increasingly unstable, more prone to “giving way”, and raises the risk of falls.
- Joint deformity and limb malalignment: Bow-legs or knock-knees may worsen over time, altering your gait pattern.
- Psychological impact: Chronic pain can lead to sleep disturbance, anxiety, depression, and reduced social engagement.
Principles of Managing Knee Osteoarthritis
The encouraging news is that, while knee osteoarthritis cannot be completely reversed, it can be effectively managed. The approach to treatment is multi-modal, personalised to the individual, and delivered in a stepwise manner:
- Foundation: Non-pharmacological treatment (education, lifestyle modification, weight management, physiotherapy).
- Step 2: Pharmacological treatment (topical and oral medications).
- Step 3: Intra-articular injections.
- Step 4: Surgery.
The main goals of treatment are to:
- Reduce pain and manage inflammation.
- Improve physical function and maintain independence.
- Slow the progression of the condition.
- Enhance overall quality of life.
Physiotherapy and Non-Pharmacological Treatment Approaches
These approaches form the most important and most effective foundation for managing knee osteoarthritis, particularly in the early-to-moderate stages. At Maple Healthcare in Ho Chi Minh City, clinicians consistently emphasise the value of these conservative, non-invasive methods.
- Education and self-management: Understanding your condition empowers you to adjust your activities, avoid harmful postures, and set realistic expectations for your recovery.
- Weight management: If you are carrying excess weight, losing 5–10% of your body weight can lead to a meaningful reduction in knee pain and a noticeable improvement in function. This is considered one of the most effective interventions available.
- Building strength in the muscles that support the knee joint (quadriceps, hamstrings, and gluteal muscles).
- Improving joint range of motion.
- Enhancing balance and coordination to reduce the risk of falls.
- Using modalities such as thermotherapy and TENS (transcutaneous electrical nerve stimulation) for pain relief. Physiotherapy: A tailored physiotherapy programme can help address all of the above goals.
- Choosing appropriate physical activity: Low-impact activities such as walking on flat surfaces, cycling, swimming, yoga, or tai chi are encouraged. Avoid high-impact activities that place sudden, jarring forces on the joint, such as running or jumping.
- Using assistive devices: In some cases, your clinician may recommend the use of a walking cane (held on the side opposite the affected knee), a knee brace, or orthopaedic insoles to help offload the joint.


Effective Exercises for People with Knee Osteoarthritis
Regular, well-guided exercise is an essential part of managing knee osteoarthritis. Always warm up thoroughly before exercising and stretch afterwards. Stop immediately if you experience sharp pain.
Warm-Up (5–10 Minutes)
Gently rotate each joint, and perform light stretches for the front of the thigh (quadriceps), the back of the thigh (hamstrings), and the calf muscles.
Strengthening Exercises
Perform 2–3 sets of 10–15 repetitions for each exercise.
- Quad Set: Lie on your back with your legs straight. Place a small rolled towel under one knee. Gently press the back of your knee down into the towel, tightening the front thigh muscle, and hold for 5 seconds before releasing.
- Straight Leg Raise: Lie on your back with one knee bent and that foot flat on the floor. Keep the other leg straight. Tighten the thigh muscle of the straight leg and slowly lift it to approximately 20–30 cm off the floor. Hold for 3–5 seconds, then slowly lower it back down.
- Glute Bridge: Lie on your back with both knees bent and feet flat on the floor. Slowly lift your hips off the floor until your body forms a straight line from your shoulders to your knees. Hold for 5 seconds, then lower back down.
- Clamshell: Lie on your side with both knees bent and stacked on top of each other. Keeping your heels together, slowly rotate your top knee upward, opening your hips. Hold for 3 seconds, then lower back down.

Range of Motion Exercises
- Heel Slide: Lie on your back with both legs straight. Slowly slide the heel of one foot towards your buttocks, bending the knee as far as is comfortable without pain. Hold for a few seconds, then slowly slide it back to the starting position.
Exercise Safety Guidelines
- Always listen to your body. Mild discomfort during exercise may be acceptable, but if you experience sharp pain or increased pain after exercise, reduce the intensity or rest.
- Avoid exercises that require bending the knee beyond 90 degrees, or any jumping or impact-based movements.
Medications Used in Knee Osteoarthritis Management
Medications can help manage symptoms, particularly during acute pain episodes. However, they are best used as part of a comprehensive treatment plan rather than as a standalone solution.
- Topical medications: Gels or creams containing NSAIDs (such as diclofenac or ibuprofen) are often the preferred first-line option due to their lower risk of systemic side effects. Capsaicin cream (derived from chilli peppers) may also help reduce pain after several weeks of consistent use.
- Paracetamol (Acetaminophen): May be used for mild pain relief, though care should be taken not to exceed the recommended maximum daily dose.
- Oral NSAIDs (Non-steroidal anti-inflammatory drugs): Medications such as ibuprofen and naproxen can be effective in reducing pain and inflammation. However, they carry a risk of side effects affecting the stomach, kidneys, and cardiovascular system. For this reason, they should be used at the lowest effective dose for the shortest duration necessary, and only under the guidance of a clinician.
- Duloxetine: An antidepressant that has also been approved for the management of chronic pain, including pain associated with osteoarthritis.
Knee Joint Injection Options
When oral medications and physiotherapy provide insufficient relief, your clinician may consider a direct injection into the knee joint.
- Corticosteroid injections: These can provide rapid reduction in inflammation and pain. The effect typically lasts from a few weeks to a few months. However, they should not be overused — generally no more than 3–4 injections per year for a single joint — as repeated injections may cause long-term cartilage damage.
- Hyaluronic acid (viscosupplementation) injections: These help restore natural lubrication within the joint, reducing friction and pain. The onset of effect is typically slower than corticosteroids but may last longer — up to 6 months or more. This option tends to be most appropriate for patients in the mild-to-moderate stages of the condition.
- Platelet-rich plasma (PRP) injections: A small amount of your own blood is drawn, processed by centrifuge to concentrate the platelets, and then injected into the joint. The evidence supporting PRP’s effectiveness is still evolving, but it may be a consideration for some younger patients in the earlier stages of knee osteoarthritis.
Surgical Options for Knee Osteoarthritis
Surgery is considered a last resort when conservative management has not been sufficient and quality of life is significantly affected.
- Knee arthroscopy: The role of arthroscopy in treating osteoarthritis is now very limited and is only indicated in carefully selected cases where a concurrent mechanical issue is present, such as a displaced meniscal fragment.
- Osteotomy (corrective bone realignment surgery): This procedure is suited to younger, active patients who have a limb malalignment (bow-legs) and osteoarthritis confined to one compartment of the knee. It works by redistributing load toward the healthier part of the joint cartilage.
- Knee replacement surgery (partial or total): This is the most effective surgical option for end-stage knee osteoarthritis (Grade 4). The damaged cartilage and bone are removed and replaced with an artificial joint. A modern knee replacement implant can generally function well for approximately 15–20 years.
Nutrition and Lifestyle Modifications
Diet and lifestyle play an important supporting role. A healthy, balanced diet not only helps with weight management but may also contribute to reducing systemic inflammation.
- An anti-inflammatory diet: Focus on foods rich in omega-3 fatty acids (salmon, sardines, flaxseed, walnuts), leafy green vegetables, colourful fruits, and wholegrains. Limit refined sugars, processed foods, and saturated fats.
- Vitamin D and calcium: Ensure adequate intake of these two nutrients to support overall bone and joint health, ideally through dietary sources where possible.
- Staying well hydrated: Water is essential for maintaining the hydration and quality of both cartilage and joint fluid.
- Supplements: Products such as glucosamine/chondroitin, type II collagen, and curcumin may offer some individuals modest benefits in reducing pain and supporting joint health. However, their effects vary between individuals and they cannot replace core treatment approaches. Always consult your clinician before starting any supplement.
- Healthy lifestyle habits: Getting adequate sleep, managing stress, and not smoking all contribute to better overall health and support the recovery process.
Daily Pain Relief Tips and Prevention Strategies
Small changes to your daily habits can make a meaningful difference over time.
- Pacing: Spread your activities throughout the day, alternating between periods of activity and rest. Avoid overexerting yourself in a single session.
- Safe movement techniques:
- On stairs: Lead with your stronger leg going up, and with your more painful leg going down. Always use the handrail.
- When standing up from a chair: Slide to the edge of the seat first, place one foot slightly behind the other, and use your arms to push yourself up.
- When lifting objects: Bend your knees, keep your back straight, and hold the object close to your body.
- Home environment modifications: Use chairs of an appropriate height, install grab rails in the bathroom, and clear walkways to reduce the risk of tripping or falling.
- Heat and cold therapy: Apply warmth (15–20 minutes) before exercise to help relax the muscles. Apply a cold pack (15 minutes) after physical activity to help reduce swelling and inflammation.

Moving Forward with Knee Osteoarthritis
Living with knee osteoarthritis is a long-term journey, but you do not have to navigate it alone. The key to managing this condition successfully lies in being proactive, consistent, and taking a comprehensive approach. The cornerstones of effective management are:
- Managing your weight.
- Exercising regularly and correctly.
- Making positive changes to your lifestyle and daily movement habits.
If you are dealing with knee pain or are unsure where to begin, please do not hesitate to seek support from a qualified specialist. At Maple Healthcare in Ho Chi Minh City, our team of clinicians and physiotherapists is ready to listen, carry out a thorough assessment, and develop a personalised management plan tailored to your needs. Our approach prioritises non-pharmacological, non-surgical methods to help you reduce discomfort, restore function, and feel confident returning to an active life.
Take the first step today. Book an appointment with us to receive personalised guidance and start building the best care plan for your knees.
FAQ: Frequently Asked Questions About Knee Osteoarthritis
Can knee osteoarthritis be cured?
Answer: Knee osteoarthritis cannot be completely reversed, as damaged cartilage does not regenerate to its original state. However, symptoms can be effectively managed, the progression of the condition can be slowed, and a good quality of life can be maintained with the right approach.
Is walking recommended for people with knee osteoarthritis?
Answer: Yes — walking is a highly beneficial form of exercise and is actively encouraged. Walk on flat surfaces, wear supportive footwear, and start with shorter distances before gradually increasing. Running is generally best avoided, as it places considerably more force on the knee joint.
Can I go to the gym or practise yoga with knee osteoarthritis?
Answer: Yes, in most cases — but exercise selection and modification are important. Avoid movements that involve deep knee bending or positions that place excessive stress on the joint. Let your instructor know about your condition so they can offer appropriate guidance and modifications.
Does cold weather make knee osteoarthritis pain worse?
Answer: Many people do report increased pain when the weather changes, which may be related to shifts in atmospheric pressure and muscle tension. To help manage this, keep your knees warm, apply heat therapy, and maintain gentle movement indoors.
Should I wear a knee brace all the time?
Answer: A knee brace can provide useful support and pain relief during activity. However, wearing it continuously throughout the day is not recommended, as this may weaken the surrounding muscles over time. It is best used selectively — for example, during periods of increased walking or exercise.
Related articles:
Contact for consultation
MAPLE INTERNATIONAL CO., LTD
Phone: 0705 100 100
Tax code: 0311948301
Date Range: 21 - 08 - 2012
Issued: Department of Planning and Investment of Ho Chi Minh City
Healthcare Group Members

Contact Us
COPYRIGHT

![]()