Developmental Dysplasia of the Hip: Signs & Diagnosis
As a parent, nothing matters more than your child’s health and overall development. So it’s completely understandable to feel concerned when you hear the term developmental dysplasia of the hip (DDH). This is a fairly common condition in newborns and young children — but the good news is that when detected early and managed appropriately, the vast majority of babies can make a full recovery and go on to achieve normal motor development.
This article, developed with input from pediatric musculoskeletal specialists, provides you with a comprehensive guide to developmental dysplasia of the hip — from recognizing early signs and understanding modern diagnostic tools such as hip ultrasound, to exploring effective treatment options like the Pavlik harness and practical advice on caring for your baby at home. Read on to learn how you can support your child on their journey to healthy growth.
Overview of Developmental Dysplasia of the Hip (DDH)
To understand this condition clearly, it helps to start with some key terminology. Developmental dysplasia of the hip (DDH) is the modern medical term used to describe a spectrum of hip abnormalities in children, including:
- Acetabular dysplasia: The mildest form, where the acetabulum (the socket of the pelvis) is shallow or incompletely formed, meaning the femoral head is not securely held in place.
- Subluxation: The femoral head is partially displaced from the center of the acetabulum.
- Complete dislocation: The femoral head sits entirely outside the acetabulum.
In the past, the term “congenital hip dislocation” was commonly used to describe more severe cases. However, DDH is the more accurate term because it captures the full range of abnormal hip development, which can occur before, during, or after birth.
Statistically, DDH occurs in approximately 1–2 per 1,000 live births. Because many cases present no obvious symptoms in the first months of life, hip screening plays a critically important role in ensuring timely intervention.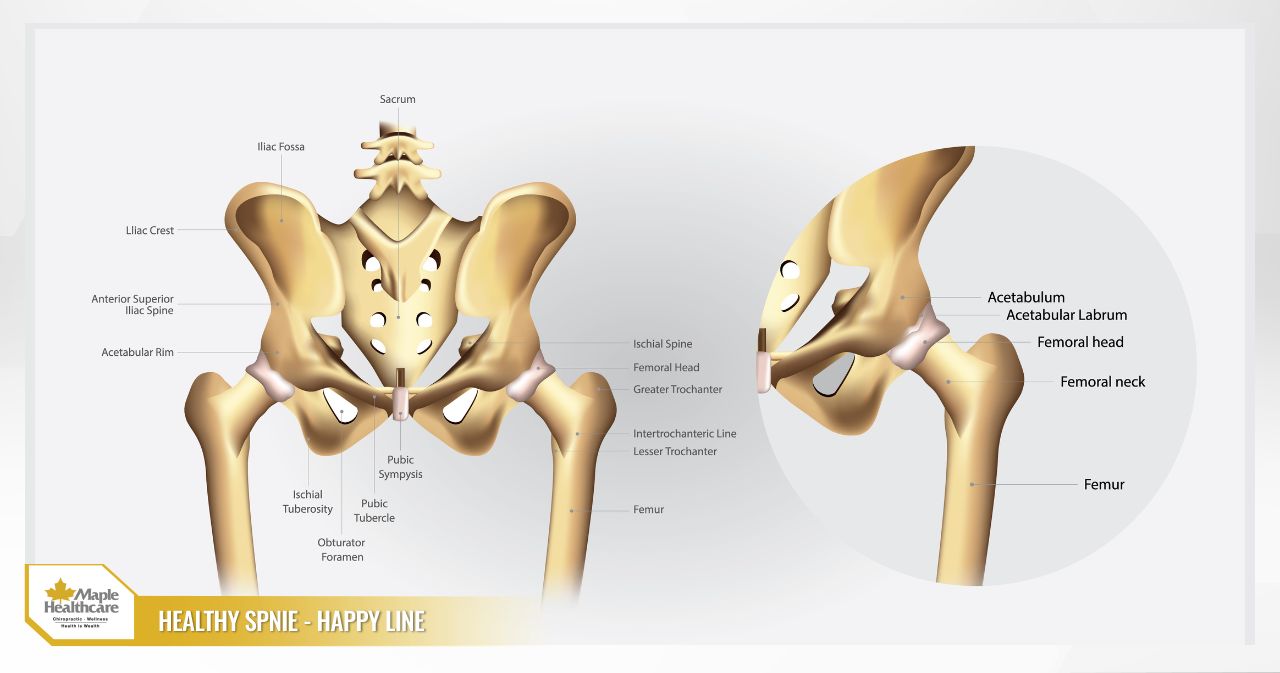
Causes and Risk Factors of Hip Dysplasia
DDH does not arise from a single cause — it is the result of multiple interacting factors. Understanding these risk factors helps both parents and clinicians take a more proactive approach to screening.
Pregnancy and Obstetric Factors
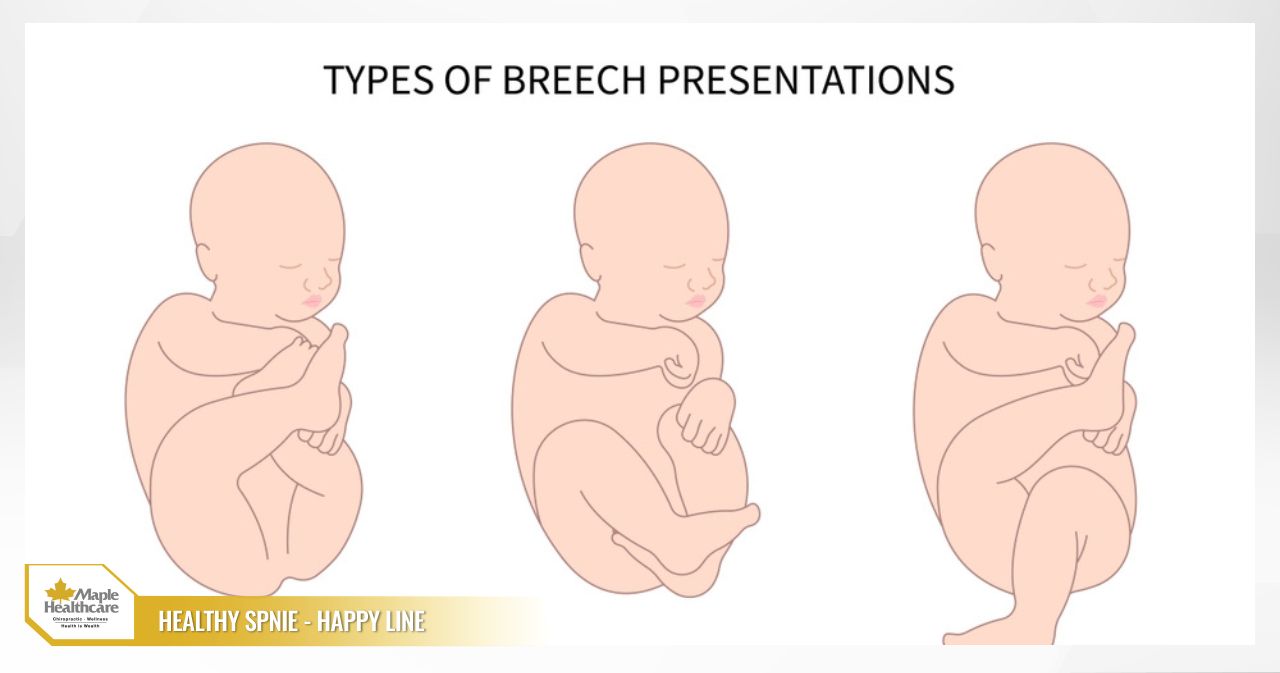
- Breech presentation: This is the single highest risk factor. The position of the baby in the womb places the hip in flexion with the knee extended, creating pressure on the joint.
- Female sex: Girls are approximately 4–8 times more likely to develop DDH than boys, possibly due to greater sensitivity to the maternal hormone relaxin, which causes ligament laxity.
- Firstborn child: A first-time mother’s uterus tends to be tighter, which limits the baby’s range of movement in the womb.
- Family history: If a parent or sibling has had DDH, the baby’s risk is higher.
- Oligohydramnios: Reduced amniotic fluid decreases space within the uterus, increasing pressure on the baby’s hips.
- Multiple pregnancy: Similar to firstborn babies, carrying multiple fetuses reduces available space in the uterus.

Postnatal and Environmental Factors
- Incorrect swaddling, carrying, or babywearing practices: Tight swaddling that forces the baby’s legs straight and together is a particularly harmful practice that can push the femoral head out of the acetabulum. This is one of the preventable contributing factors.
- Non-hip-healthy positions: Any position that forces the baby’s legs into prolonged extension and adduction is considered unfavorable for healthy hip development.
Associated Medical Conditions
- Connective tissue disorders: Conditions such as Ehlers-Danlos syndrome cause generalized ligament laxity throughout the body, including the hip ligaments.
- Abnormal muscle tone: Certain neuromuscular conditions can also affect hip joint stability.
Developmental dysplasia of the hip can affect one or both hips. Bilateral cases — where both hips are involved — can be more subtle and harder to identify because there is no obvious asymmetry to compare between the two sides.
Signs of Developmental Dysplasia of the Hip by Age Group
Observing your baby closely every day is one of the best ways to detect any early abnormalities. The signs to look out for vary depending on your child’s age.
Ages 0–3 Months
- Asymmetric skin folds on the buttocks and thighs: With your baby lying face down, observe the skin creases on the buttocks and the back of the thighs. If the number, position, or depth of these folds differs between the two legs, this may be a sign worth investigating.
- Limited hip abduction: This is an important sign. You may notice during nappy changes that one hip is more difficult to open outward (abduct) than the other.
- A clicking or clunking sensation at the hip: In some cases, you may hear or feel a distinct “clunk” when moving your baby’s leg.
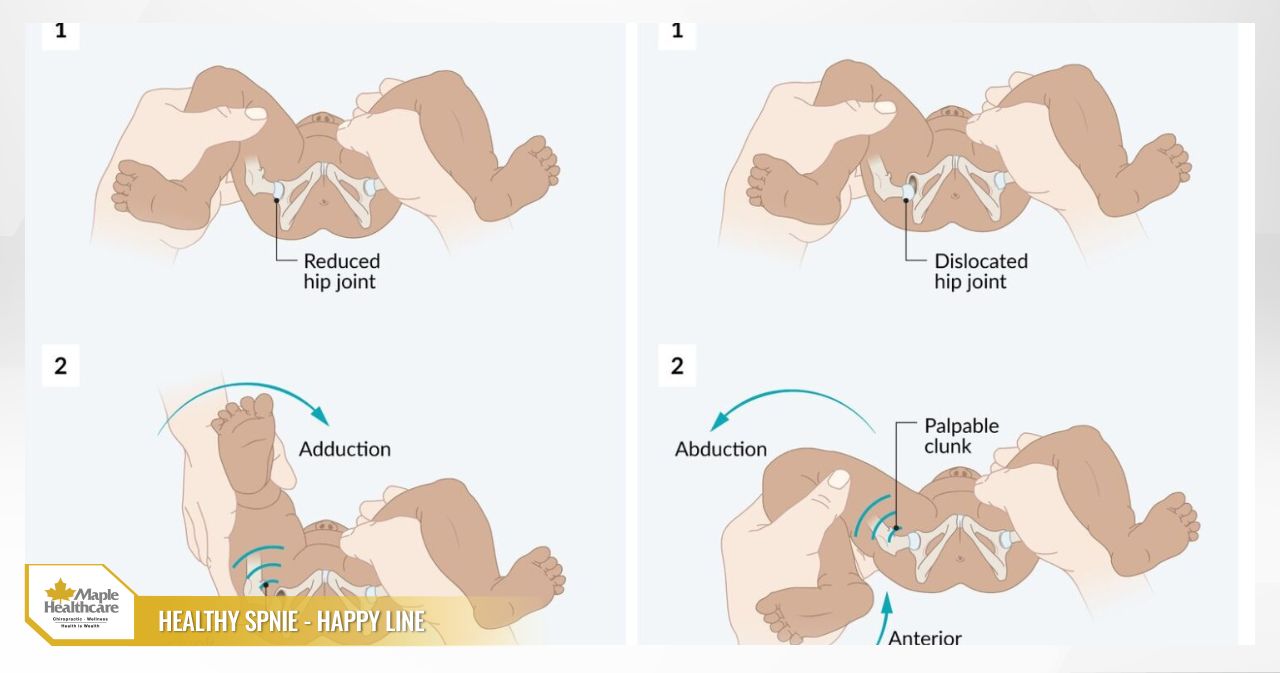
- Ortolani and Barlow tests: These are clinical examinations performed by a doctor to assess hip joint stability. A positive result means the clinician can feel the femoral head dislocating from or being reduced back into the acetabulum.
Ages 3–12 Months
- Leg length discrepancy (Galeazzi sign): With your baby lying on their back, bend both knees and place both feet flat on the surface. If one knee appears lower than the other, this may indicate that the leg on that side is effectively shorter due to hip dislocation.
- Limited hip abduction becomes more noticeable.
- The baby may tend to rotate the affected leg outward.
Once the Child Begins to Stand and Walk (>12 Months)
- Limping or a waddling gait (Trendelenburg gait): If only one hip is affected, the child will walk with a limp. If both hips are involved, they may walk with a characteristic waddling pattern, similar to a duck.
- Functional scoliosis: The body may tilt to one side to compensate for the shorter leg.
- Increased lordosis (an exaggerated inward curve of the lower back).
Important note: DDH is typically painless in newborns and infants. Cases where both hips are affected may not show any asymmetry, making detection even more challenging.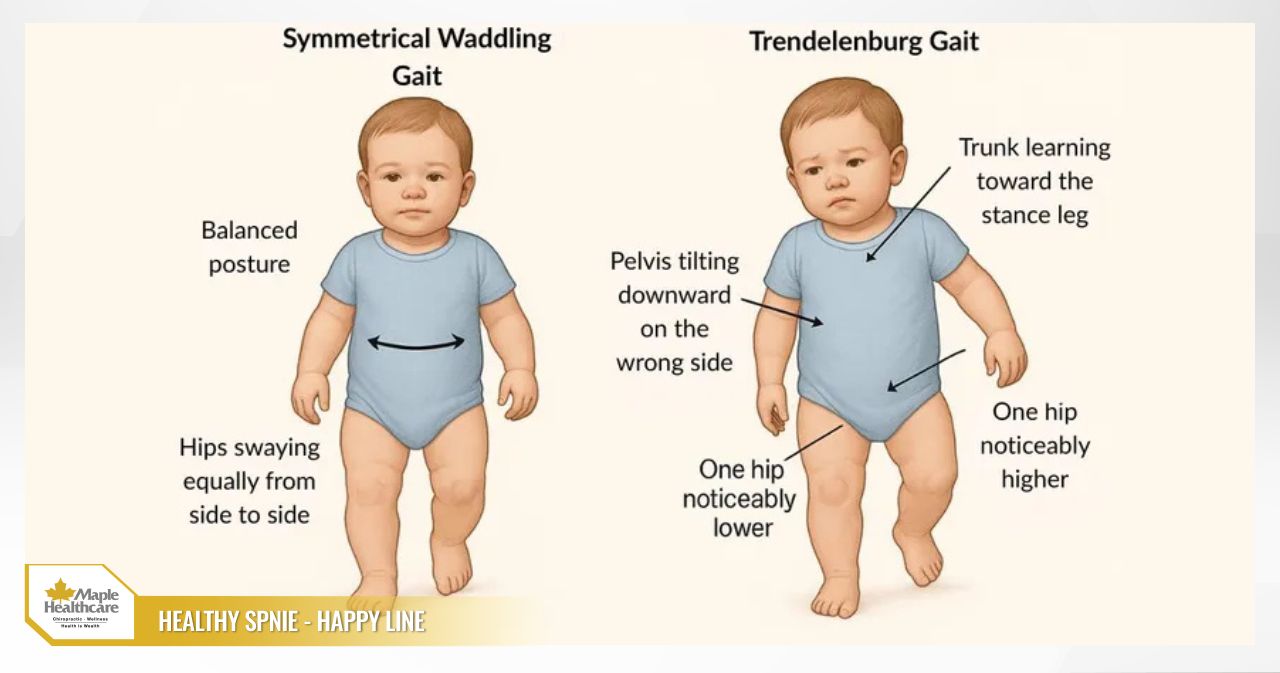
When Should You Bring Your Child in for Assessment?
Proactive parental awareness is the most valuable tool in early detection. You should bring your baby to a pediatric or pediatric orthopedic specialist as soon as you notice:
- Any of the signs described above, even if they seem minor.
- Your baby falls into a high-risk group (breech birth, family history of DDH, female sex, or firstborn child).
According to current clinical recommendations, hip ultrasound screening at 4–6 weeks of age is indicated for all babies with risk factors, and in many countries is offered as a routine check for all newborns.
Red flag signs that warrant prompt medical attention:
- Unable to comfortably abduct (open out) your baby’s hip during nappy changes.
- Clearly hearing or feeling a clicking or clunking sensation at your baby’s hip.
- One leg appearing visibly shorter than the other.
- Your baby showing unusual delays in reaching motor milestones such as standing or walking.
Diagnosing Developmental Dysplasia of the Hip Accurately
To confirm a diagnosis, in addition to taking a full history and reviewing risk factors, your clinician will perform a physical examination and arrange appropriate imaging investigations.
Clinical Examination
Your doctor will carefully assess your baby’s hips, including:
- Performing specialized tests such as the Ortolani and Barlow maneuvers (which are only clinically meaningful in babies under 3 months of age).
- Assessing the range of hip abduction on both sides.
- Checking the Galeazzi sign to compare the relative leg lengths.
- Observing skin fold symmetry and leg positioning.
Imaging Investigations
Imaging is the definitive tool for diagnosing and classifying the severity of DDH.
Hip Ultrasound in Newborns (Ages 0–6 Months)
- This is the gold standard for diagnosing DDH in young infants, because the femoral head and acetabulum at this age are predominantly cartilaginous and are not clearly visible on X-ray.
- The technique is safe and does not involve radiation.
- Clinicians use the Graf classification system, which is based on measuring the alpha and beta angles to evaluate the depth of the bony acetabular roof and the coverage provided by the cartilaginous roof. A low alpha angle combined with a high beta angle indicates a shallow socket and an unstable hip joint.
Hip X-Ray (Children Older than 4–6 Months)
- Once the ossification center of the femoral head has appeared, X-ray becomes a more useful tool.
- Your clinician will analyze the X-ray using established reference lines and indices, including:
- Acetabular Index (AI): This measures the angle of the acetabular roof. An AI higher than expected for the child’s age is a marker of dysplasia.
- Hilgenreiner’s line and Perkin’s line: These help determine the position of the femoral head relative to the acetabulum.
- Shenton’s arc: A smooth, continuous curve connecting the femoral neck and the pelvis. If this arc is broken, it suggests subluxation or dislocation.
These screening and diagnostic programs follow international recommendations from authoritative bodies such as the American Academy of Pediatrics (AAP), ensuring that all children are systematically evaluated.
What Does DDH Classification and Severity Mean for Your Child?
Classifying the severity of DDH — particularly through the Graf ultrasound grading system — is directly relevant to guiding treatment decisions and predicting outcomes.
- Graf Type I: Normal, mature hip joint.
- Graf Type IIa: Physiologically immature hip (acceptable in babies under 3 months); monitoring is recommended.
- Graf Type IIb: Mild dysplasia (in babies over 3 months); treatment should be initiated.
- Graf Type IIc/D: Severe dysplasia with a hip at risk of dislocation; immediate treatment is required.
- Graf Type III & IV: Dislocated hip; active intervention is necessary.
As a general principle: the more severe the dysplasia, the more urgently and comprehensively treatment needs to be addressed.
Effective Treatment Options for Developmental Dysplasia of the Hip
The primary goal of treatment is to guide the femoral head back into its correct, centered position within the acetabulum and maintain that stability so the hip joint can develop normally. The appropriate treatment approach depends closely on the child’s age and the severity of the condition.
Ages 0–6 Months: The Pavlik Harness
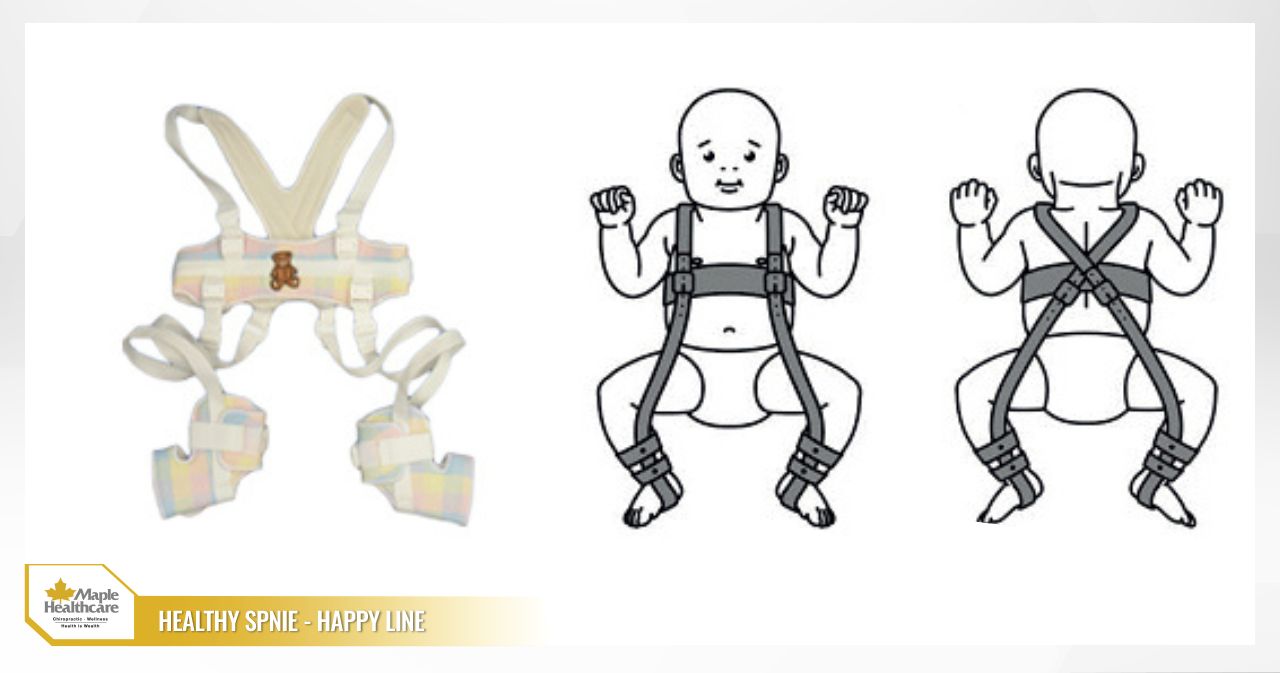
- This is the most widely used, gentle, and effective treatment for young babies.
- How it works: The Pavlik harness is a soft harness system that holds both hips in a flexed and abducted position (similar to a frog-leg posture). This position naturally directs the femoral head deeper into the acetabulum, encouraging the socket to develop with greater depth and roundness.
- How it is used: Your baby will typically wear the harness for approximately 23 hours per day over a period of 6–12 weeks. Your clinician will guide you on how to care for and adjust the harness. Regular follow-up appointments and ultrasound checks will be scheduled to monitor progress.
- Success rates: Very high (above 90%) when the condition is identified early and the harness is worn consistently as advised.
Ages 6–18 Months: Closed Reduction and Spica Casting
- As children grow older, the Pavlik harness may no longer be sufficient.
- The procedure: The child is given a general anaesthetic to allow full muscle relaxation. The clinician then manually guides the femoral head back into the acetabulum (closed reduction). Once the correct position has been confirmed — sometimes using an arthrogram (contrast X-ray) — the child is placed in a special type of cast called a Spica cast, which immobilizes the pelvis and both thighs in an abducted position.
- Duration: The cast is typically worn for approximately 3 months and may need to be changed during this period.
Over 18 Months or When Other Methods Have Not Been Successful: Surgery
- If DDH is identified late or if conservative methods have not achieved a stable, well-positioned hip, surgery becomes necessary.
- Types of surgical procedures:
- Open reduction: The surgeon makes an incision to access the joint directly, removes any obstructing tissue, and repositions the femoral head into the acetabulum.
- Osteotomy: In many cases, bone procedures are also required to correct structural deformities. Commonly performed surgeries include pelvic osteotomies (Salter, Pemberton, Dega) to reorient and improve coverage of the acetabulum, as well as femoral osteotomy to correct the alignment of the femur.
- Following surgery, the child will again be placed in a Spica cast, followed by a period of physiotherapy and rehabilitation.
Home Care and Monitoring: The Role of Parents
Family involvement is an indispensable part of a successful treatment journey.
While Your Baby Is in a Pavlik Harness or Spica Cast
- Skin care: Keep your baby’s skin clean and dry at all times, particularly around the areas beneath the straps or at the cast edges, to prevent rashes or skin breakdown. Carefully tuck a nappy underneath the harness or cast.
- Bathing: Use sponge baths rather than full immersion. Do not remove the Pavlik harness without explicit instruction from your clinician.
- Monitoring: Watch for any concerning signs such as redness or swelling of the skin, a bluish or pale color, cold limbs, persistent or unusual crying, or an unpleasant odor from the cast — and report these to your doctor promptly.
Applying “Hip-Healthy” Positioning Principles
These principles are important for ALL newborns, regardless of whether they have been diagnosed with DDH.
- When swaddling: Only wrap the upper body. Leave both legs free to move, bend, and flex naturally.
- When carrying or using a baby carrier: Always ensure your baby’s hips are in a flexed and abducted position (an “M” shape or frog-leg posture), with the knees level with or higher than the bottom. Avoid carriers that allow the baby’s legs to hang straight down.
Regular Follow-Up
It is important to attend all scheduled follow-up appointments and to complete any recommended imaging as directed, to ensure your baby’s hip joint is developing on a stable trajectory.
Complications and Outlook Without Treatment
If developmental dysplasia of the hip is not identified and treated in a timely manner, the consequences as the child grows can be significant:
- Permanent leg length discrepancy.
- A persistent limp or abnormal gait pattern.
- Chronic hip pain.
- Restricted mobility, affecting the ability to participate in sports and daily activities.
- Early-onset hip osteoarthritis: This is the most serious long-term complication, which may require total hip replacement at a relatively young age.
On the other hand, the outlook is generally very positive when DDH is diagnosed and treated within the first six months of life. Most babies go on to develop a normally functioning hip joint without any long-term problems. The later the diagnosis, the more complex the treatment and the greater the risk of lasting complications.
Prevention and Screening for Hip Dysplasia
While it is not always possible to prevent the underlying developmental factors, you can help reduce risk and support early detection through:
- Parental education: Raising awareness of hip-healthy care practices, particularly correct swaddling and babywearing techniques.
- Systematic screening programs: Obstetricians and pediatricians should work together to identify at-risk infants and arrange timely hip ultrasound screening. Establishing standardized care pathways based on best-practice guidelines — such as those from the National Institute for Health and Care Excellence (NICE) in the UK — is essential.
- Family observation: As a parent, you know your baby best. Trust your instincts and do not hesitate to raise any concerns with your doctor.
FAQ: Common Questions About Developmental Dysplasia of the Hip
Does DDH cause pain in babies? Can it resolve on its own?
Answer: In the newborn period, DDH is typically painless. The condition very rarely resolves without intervention and tends to worsen over time if left unmanaged. Monitoring and treatment as directed by your clinician is essential.
How long does a baby wear the Pavlik harness? Can they still be bathed and vaccinated?
Answer: The harness is typically worn for 6–12 weeks. Vaccinations can proceed as normal. Bathing is done using sponge baths to keep the harness dry, unless your clinician specifically advises that it may be temporarily removed.
After treatment, when will my baby be able to crawl and walk normally? Will physiotherapy be needed?
Answer: Most children who are successfully treated go on to reach their motor development milestones in line with their peers. In some cases — particularly following surgery — your clinician may recommend pediatric physiotherapy exercises to help rebuild muscle strength and restore range of movement.
Is DDH hereditary? If one of my children has been diagnosed, what should I do in a future pregnancy?
Answer: There is a familial component to DDH. If you have had a child diagnosed with the condition, please inform your obstetrician at the start of your next pregnancy. Any subsequent babies will need careful hip screening shortly after birth.
If DDH is identified late (after 1–2 years of age), can it still be treated effectively?
Answer: Treatment is still possible, but it becomes considerably more complex and almost always requires surgery, with a longer recovery period. Outcomes depend heavily on the child’s age and the degree of dislocation at the time of diagnosis.
Caring for a child with developmental dysplasia of the hip calls for patience and close collaboration between your family and the healthcare team. Try not to let worry become overwhelming.
If your baby has any risk factors, we encourage you to proactively arrange a hip ultrasound screening appointment at 4–6 weeks of age.
Take time to learn about “hip-healthy” care practices to support your baby’s delicate hip joints every single day.
If you notice any warning signs, please get in touch with our orthopedic specialists at Maple Healthcare in Ho Chi Minh City for early advice and assessment. Early detection of developmental dysplasia of the hip is one of the most meaningful investments you can make in your child’s long-term health.
Related articles:
Contact for consultation
MAPLE INTERNATIONAL CO., LTD
Phone: 0705 100 100
Tax code: 0311948301
Date Range: 21 - 08 - 2012
Issued: Department of Planning and Investment of Ho Chi Minh City
Healthcare Group Members

Contact Us
COPYRIGHT

![]()