Patellar Tendinitis: Everything You Need to Know
Are you a fan of sports like basketball, volleyball, or running? Do you often feel a sharp pain at the front of your knee, just below the kneecap, after high-intensity training sessions? If so, there is a good chance you are dealing with patellar tendinitis — also known as “Jumper’s knee.” This is a very common overuse injury that causes a dull, persistent ache at the front of the knee and can significantly impact both athletic performance and everyday activities.
The good news is that most cases of patellar tendinitis can be effectively managed and rehabilitated through training load adjustments, a structured rehabilitation exercise program, and a few lifestyle changes.
This article, developed with input from clinicians at Maple Healthcare, is your comprehensive A-to-Z guide to understanding this condition — from its root causes and how to recognise its symptoms, to accurate diagnostic methods and a detailed, phase-by-phase treatment and exercise plan for patellar tendinitis. Let us help you manage the pain, rebuild tendon strength, and return to the sport you love as safely as possible.
What Is Patellar Tendinitis?
To understand this injury, let us first take a brief look at the anatomy involved.
Anatomy and How It Works
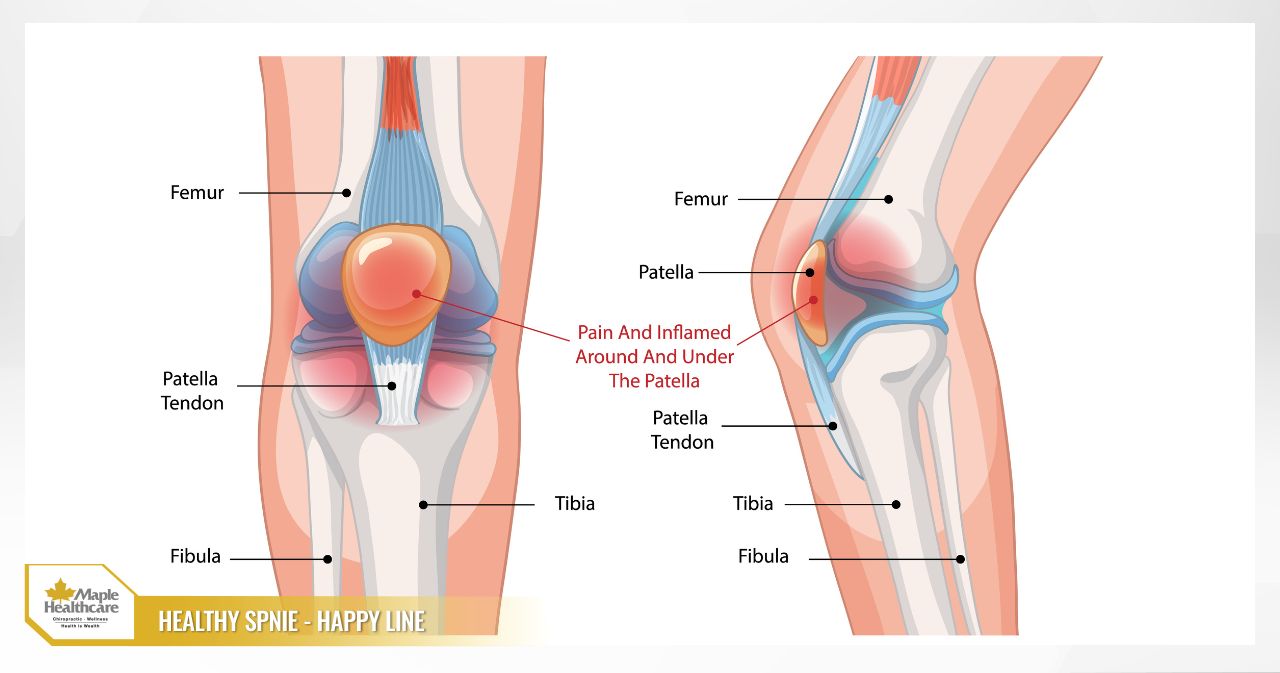
The patellar tendon is a strong, fibrous band of connective tissue that connects the lower pole of the kneecap (patella) to the tibial tuberosity — the bony prominence at the top front of the shin.
This tendon plays an essential role in transferring force from the quadriceps muscle group (the large muscle at the front of the thigh) down to the lower leg. This mechanism allows us to perform movements such as straightening the knee, walking, running, climbing stairs, and — especially — explosive movements like jumping and landing. When you jump and land, the patellar tendon must absorb a very large tensile force, sometimes many times your body weight.
Terminology: Tendinitis or Tendinopathy?
Although the condition is commonly called “patellar tendinitis,” the more clinically precise term in chronic cases is patellar tendinopathy. This is because histological studies show that the primary damage involves structural degeneration of the tendon (disrupted and disorganised collagen fibres) caused by repeated microscopic tears that do not have sufficient time to heal — rather than a classic acute inflammatory response. This condition tends to progress into persistent, dull pain and functional decline over time.
- Acute: Typically has a sudden onset following an excessively intense training session or a specific injury.
- Chronic: Pain persists for weeks or months, usually as a result of gradual overloading that has not been appropriately managed.
Typical Symptoms of Patellar Tendinitis
Recognising the signs early is key to timely intervention and preventing the injury from becoming more serious. Below are the most common symptoms:
- Localised, well-defined pain: Anterior knee pain concentrated at a single point, just below the kneecap (the inferior pole). You can typically point to the exact location with one finger.
- Pain that worsens with activity: The pain becomes worse when performing activities that place stress on the tendon, including: jumping and sprinting; going up or down stairs and slopes; squatting or performing lunge exercises; and sitting for extended periods with the knee bent.
- Morning stiffness: A feeling of stiffness and discomfort in the knee upon waking, which typically improves after a few minutes of light movement.
- Mild swelling and tenderness to touch: There may be mild swelling around the tendon area and pain when pressing on it.
- Quadriceps weakness: Because the body adopts a “protective” response to avoid pain, the quadriceps muscle may gradually weaken, reducing athletic performance.
Warning signs that require immediate medical attention: If you experience severe symptoms such as persistent pain even at rest, notable swelling, or significant weakness in the knee, these may indicate a more serious injury. Continuing to train through these warning signs may increase the risk of a complete patellar tendon rupture — a serious injury requiring urgent medical care.
Causes of Patellar Tendinitis and Risk Factors
Patellar tendinitis rarely results from a single event. It is the product of accumulated, repetitive stress on the tendon. The main contributing causes include:
- Overloading and training errors: This is the leading cause. It includes increasing training volume, frequency, or intensity too quickly; switching from soft to hard training surfaces; and using worn-out or ill-fitting footwear.
- Biomechanical factors and muscle imbalances: The way your body moves also plays an important role. Issues such as tight or weak quadriceps, weak gluteal and hamstring muscles, restricted ankle dorsiflexion, or poor landing technique all increase the load placed on the patellar tendon.
- Individual factors: The condition is most common in adolescents and young adults (ages 15–30). Being overweight and having a previous history of knee injury are also recognised risk factors.

How Patellar Tendinitis Is Diagnosed
To reach an accurate diagnosis and rule out other causes of knee pain, the doctors and physiotherapy specialists at Maple Healthcare will carry out a comprehensive assessment process:
- Medical history and clinical examination: The clinician will ask detailed questions about your symptoms and activity history, and will perform functional tests such as palpating the tender point, the decline squat test, and assessing the strength and range of motion of the relevant muscle groups.
- Diagnostic imaging (where necessary): Doppler ultrasound is a very useful tool for visualising tendon structure and detecting tendon thickening or degeneration. MRI is indicated for more complex cases. X-ray is primarily used to exclude bony problems.
- Outcome scores and differential diagnosis: The VISA-P score is used to assess pain levels, function, and to monitor treatment progress. The diagnosis must be differentiated from other conditions such as patellofemoral pain syndrome, Osgood-Schlatter disease, and Hoffa’s fat pad impingement.
Treating Patellar Tendinitis: A Phase-by-Phase Approach
The primary goals of treatment are to reduce pain, restore the tendon’s load-bearing capacity, improve strength and movement mechanics, and ultimately help you return to activity safely. The treatment plan should be individualised and progress through clearly defined phases.
Acute Phase: Pain Relief and Load Management
This phase focuses on calming the tendon and preventing the condition from worsening.
- Relative rest: Reduce activity to a level that does not provoke pain, and substitute with low-impact alternatives such as swimming or light cycling.
- Ice therapy: Apply an ice pack to the painful tendon area for 10–15 minutes after activity.
- Supportive aids: Using a patellar strap or Kinesio taping may provide temporary pain relief during activity.
Rehabilitation Phase: Controlled Loading and Tendon Capacity Rebuilding
This is the most important phase. The goal is to stimulate the tendon to repair itself and become stronger through specialised patellar tendinitis exercises.
- Isometric exercises: These provide immediate pain relief and serve as an excellent starting point.
- Eccentric exercises: The decline squat, focusing on a slow, controlled lowering phase, is used to stimulate collagen regeneration.
- Heavy Slow Resistance (HSR) training: This is the most evidence-supported approach for chronic tendinopathy, using exercises such as the leg press and weighted squats performed with heavy loads at a slow tempo.
- Stretching and movement correction: Stretching tight muscles and working with a specialist to correct movement technique faults.
Medical Interventions (When Conservative Treatment Is Insufficient)
For chronic cases that have not shown meaningful improvement after 3–6 months of active conservative treatment, other interventions may be considered.
- Extracorporeal Shockwave Therapy (ESWT): Uses high-energy sound waves to stimulate the healing process.
- Platelet-Rich Plasma (PRP) injection: May support the tendon repair process.
- Corticosteroid injection: Use with great caution. This approach is generally not recommended due to the risk of tendon weakening and rupture.
Patellar Tendon Surgery
Patellar tendon surgery is a last resort, considered only after at least 6–12 months of active conservative treatment has not been successful. Surgery typically involves the removal of degenerated tissue within the tendon. Recovery following surgery generally takes between 4–6 months.
Sample Rehabilitation Exercise Plan for Patellar Tendinitis
The golden rule: Pain during exercise is acceptable up to a level of ≤3/10 and must return to its baseline level within 24 hours. Always prioritise correct technique over repetition count.
Please note: This is a sample reference plan. You should consult a doctor or physiotherapist for a personalised programme tailored to your specific condition.
Weeks 1–2: Pain Reduction and Muscle Activation
- Isometric Quads: Sit with your leg straight, contract the quadriceps firmly, and hold for 45–60 seconds. Repeat 5 times, 1–2 times per day.
- Bridging (Glute Bridge): Lie on your back, bend your knees, and lift your hips. 3 sets × 15 repetitions.
- Side-lying Hip Abduction: 3 sets × 15 repetitions each side.
Weeks 3–6: Building Strength and Tendon Capacity
- Eccentric Decline Squat: Stand on a decline board and slowly lower yourself on one leg over 3–4 seconds. 3 sets × 15 repetitions.
- Heavy Slow Resistance (HSR): Perform leg press or weighted squats with a tempo of 3 seconds down and 3 seconds up. 3–4 sessions per week.
- Stretching: Stretch the quadriceps, hamstrings, and calf muscles. Hold each stretch for 30–45 seconds, 3 times per day.
Weeks 7–10+: Functional and Plyometric Training
- Plyometrics (Jump Training): Begin with low-intensity activities such as two-footed jumping on the spot and stepping up onto a low box. Gradually increase intensity.
- Interval Running: Begin returning to running with short intervals alternated with walking, closely monitoring your tendon’s response.
Returning to Sport After Patellar Tendinitis
Do not rush! Returning to the field too soon is one of the leading causes of recurrence. Use the following objective criteria as your guide:
- VISA-P score: Above 90 out of 100.
- Pain level: No pain during daily activities and ≤2/10 during sport-specific activities.
- Strength and function: Strength and jump performance on the affected side must reach at least 90% of the unaffected side.
- Post-exercise response: No increase in pain or swelling the morning after a demanding training session.
The time needed to meet these criteria varies considerably between individuals — typically 8–12 weeks with effective conservative treatment, and potentially 4–6 months following surgery.
How to Prevent Patellar Tendinitis From Recurring
Recovery is only half the journey. Maintaining tendon health is an ongoing process.
- Smart load management: Listen to your body, increase load by no more than 10% per week, and include adequate rest days.
- Comprehensive strength training programme: Strengthen the gluteal muscles, hamstrings, and core (trunk) muscles as well.
- Maintain flexibility: Regularly stretch and work on improving ankle joint mobility.
- Optimise technique: Pay attention to “soft” landing mechanics and controlled movement to prevent the knee from collapsing inward.
- Equipment and lifestyle: Use appropriate footwear, maintain a healthy body weight, and ensure adequate sleep.

Common Questions Answered
- Do I need to rest completely? No. Complete rest can actually weaken the tendon. It is advisable to maintain gentle, pain-free activities.
- Should I use ice or heat? Ice is effective during the acute phase. Heat may be helpful during the rehabilitation phase to relax the muscles before exercise.
- When should I see a doctor and get an ultrasound or MRI? If the pain has persisted for more than 2 weeks, or if you have more severe signs such as significant swelling, redness, or intense pain.
- What warning signs indicate a patellar tendon rupture requiring emergency care? A sudden “pop” or “snap” sound, followed by intense, immediate pain, rapid swelling, and the inability to straighten the knee.
Common Mistakes to Avoid During Treatment
- Resting for too long, which weakens the tendon and surrounding muscles.
- Returning to heavy activity too quickly as soon as the pain subsides.
- Only stretching while neglecting tendon-strengthening exercises (HSR, plyometrics).
- Over-relying on pain medication to mask discomfort and continue training.
Action Checklist for This Week
If you are currently experiencing pain from patellar tendinitis, here are some steps you can take right away:
- Reduce your load: Immediately cut your training volume by 20–50%.
- Keep a pain diary: Record your pain level (0–10 scale) each day to monitor changes.
- Start isometric exercises: Perform isometric quad contractions daily to help manage pain.
- Apply ice: Ice the painful tendon area after each activity session.
- Make a plan: Book an appointment with a physiotherapist to be properly assessed and to receive a personalised exercise programme.
Begin Your Recovery Journey at Maple Healthcare
Patellar tendinitis is a complex condition, and the key to managing it successfully lies in a personalised rehabilitation programme carried out with consistency. Relying solely on rest or pain medication does not address the underlying mechanical cause — a reduction in the tendon’s ability to tolerate load.
At Maple Healthcare in Ho Chi Minh City, our team of international doctors and physiotherapy specialists understands this well. We focus not only on relieving your symptoms, but also on identifying and addressing underlying contributing factors such as muscle imbalances, biomechanical irregularities, and suboptimal movement patterns.
By combining advanced, non-invasive, non-surgical conservative treatment methods — including chiropractic care, specialised physiotherapy, and rehabilitation — the clinicians at Maple Healthcare aim to support you through a comprehensive recovery plan for patellar tendinitis.
Do not let knee pain hold you back from an active life and the sport you are passionate about. Let the specialists at Maple Healthcare support you on your path to rebuilding strength and returning to play — feeling stronger than before.
Book a consultation with a specialist at Maple Healthcare today!
FAQ: Frequently Asked Questions About Patellar Tendinitis
Is Patellar Tendinitis Serious, and Why Is Early Treatment Important?
Answer: Patellar tendinitis is not life-threatening in itself, but if it is not managed appropriately and you continue to train through it, it can become chronic, significantly reducing athletic performance and quality of life. In rare cases, prolonged damage can weaken the tendon and increase the risk of a complete patellar tendon rupture — a serious injury that requires surgery.
Do I Need to Rest Completely When I Have Patellar Tendinitis?
Answer: No. Clinicians recommend “relative rest” rather than complete rest. Complete inactivity can lead to weakening of both the tendon and the surrounding muscles. You should reduce or modify activities that provoke pain (such as jumping and running) and replace them with pain-free alternatives like swimming or gentle cycling, to maintain your fitness while supporting the recovery process.
Which Exercises Are Most Important for Recovering From Patellar Tendinitis?
Answer: There is no single “best” exercise. An effective rehabilitation programme typically progresses through stages: 1) Isometric exercises to help manage pain; 2) Heavy Slow Resistance (HSR) and eccentric exercises to rebuild and strengthen tendon tissue; 3) Plyometric (jump training) exercises to prepare for a return to sport.
Will Wearing a Patellar Strap Cure Patellar Tendinitis?
Answer: A patellar strap can be a useful supportive tool for temporarily reducing pain during activity. It works by redistributing the load across the tendon. However, it is not a cure. It does not address the underlying mechanical cause — reduced tendon load tolerance. You will still need to complete a rehabilitation exercise programme to properly address the problem.
Related articles:
Contact for consultation
MAPLE INTERNATIONAL CO., LTD
Phone: 0705 100 100
Tax code: 0311948301
Date Range: 21 - 08 - 2012
Issued: Department of Planning and Investment of Ho Chi Minh City
Healthcare Group Members

Contact Us
COPYRIGHT

![]()