Scoliosis in Children: Early Warning Signs and Safe Treatment Options
Watching your child grow up is one of the greatest joys of parenthood. Yet during the rapid growth phase of adolescence, certain health concerns can quietly emerge — one of which is scoliosis in children. This is a condition where the spine curves abnormally to one side, forming a C- or S-shape, and it is most commonly seen in children between the ages of 10 and 15. While it can understandably be a source of concern, early detection and appropriate management mean that this condition can often be well-controlled.
Early detection plays a critical role. It can help prevent more severe spinal and chest deformity, and reduce the risk of longer-term complications such as cardiac and respiratory compression, chronic back pain, and the psychological impact of changes in appearance. This article is designed as a practical guide for parents — covering how to recognise early signs, what the diagnostic process involves, available treatment options including physiotherapy, bracing, and surgery, and how to support your child at home.
What Is Scoliosis in Children?
To understand scoliosis, picture the spine as a straight vertical line when viewed from behind. Scoliosis in children occurs when that line curves to one side, accompanied by a slight rotation of the vertebrae. Medically, the condition is confirmed when the angle of curvature measured on an X-ray — known as the Cobb angle — is 10 degrees or greater.
The curve may take one of two forms:
- C-shape: A single curve, typically in the thoracic (mid-back) or lumbar (lower back) region.
- S-shape: Two opposing curves that develop as the body attempts to maintain balance.
If left unaddressed, a progressive curve can lead to significant postural imbalance and trunk deformity. In more severe cases, chest wall deformity may reduce lung capacity, leading to breathing difficulties and affecting cardiovascular function.
There are three main types of scoliosis:
Idiopathic Scoliosis: This is the most common type, accounting for approximately 80% of adolescent cases — particularly what is referred to as adolescent idiopathic scoliosis. “Idiopathic” means the exact cause has not been clearly identified, although research suggests a genetic component may be involved.
Congenital Scoliosis: This type results from vertebral abnormalities that develop while the baby is still in the womb. The vertebrae may fail to form fully or separate properly, meaning the spinal curvature is present from birth.
Neuromuscular Scoliosis: This form occurs as a consequence of conditions affecting the nervous system and muscles — such as cerebral palsy, muscular dystrophy, or spina bifida. Weakness or imbalance in the muscles that support the spine means the spine is unable to maintain an upright position.
Signs and Symptoms of Scoliosis in Children
One of the key challenges with idiopathic scoliosis is that it is often painless in the early stages, which can make it difficult to detect. However, parents can look for visible signs of asymmetry at home — particularly during the adolescent growth spurt.
How to Check at Home
You can carry out a simple check by asking your child to remove their shirt and observing their back in two positions: standing upright and bending forward.
When your child is standing upright, look for the following signs of asymmetry:
- Uneven shoulders: One shoulder appears higher than the other.
- Prominent shoulder blade: One shoulder blade sticks out more noticeably than the other.
- Uneven waist: One side of the waist appears higher or fuller.
- Tilted hips: One hip sits higher than the other.
- Head not centred over the hips: The body’s midline appears to shift to one side.
- Apparent leg length difference: Because of hip tilt, one leg may appear longer than the other.
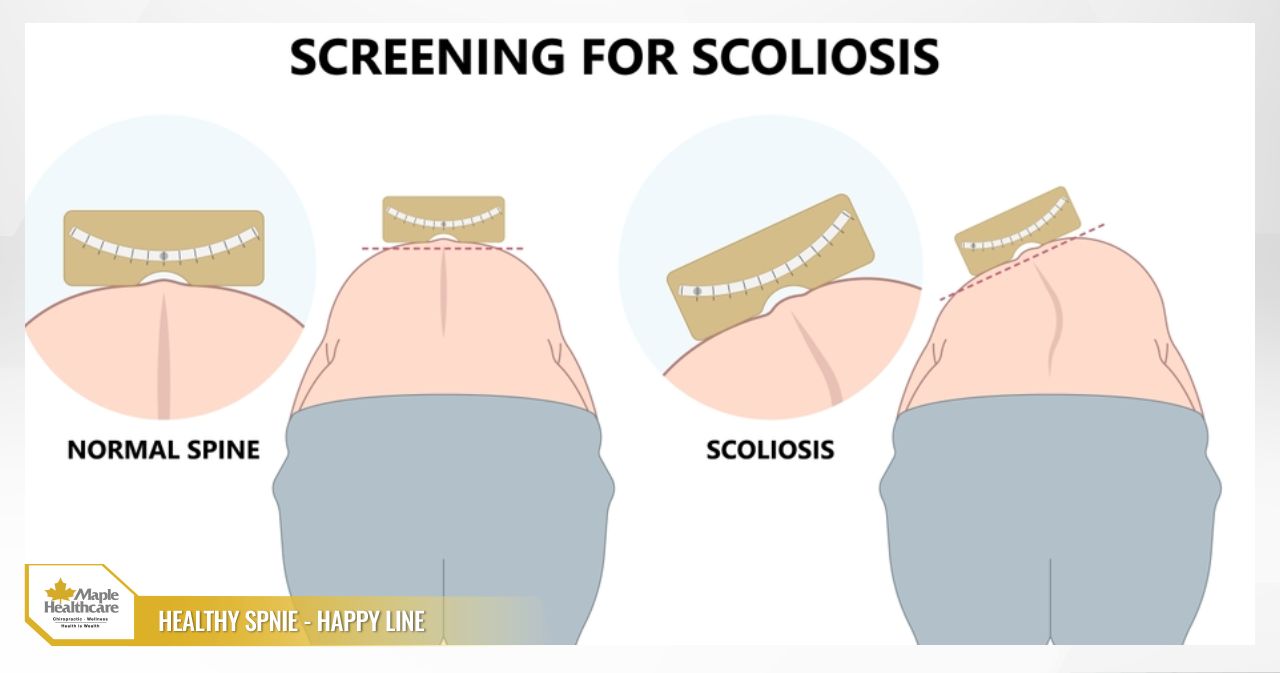
The Adam’s Forward Bend Test
This is one of the simplest and most effective scoliosis screening methods you can do at home:
- Ask your child to stand upright with feet together or shoulder-width apart.
- Have them slowly bend forward with arms hanging down, palms pressed together, reaching toward their toes — keeping their knees straight.
- Observe their back from behind. If one side of the back — particularly around the rib area — appears higher than the other, forming a visible “rib hump,” this is a notable sign that warrants further evaluation.
When Should You Seek Medical Assessment?
You should bring your child to a musculoskeletal specialist if you notice:
- Any of the asymmetries described above, even if subtle.
- Your child complains of persistent back pain or muscle fatigue.
- Neurological symptoms such as muscle weakness or numbness and tingling in the limbs — these may indicate an underlying neuromuscular cause that requires early investigation.
A practical tip: Take a photo of your child’s back while they are standing upright every 3 to 6 months. This makes it easier to compare over time and spot even small changes.
Diagnosis and Treatment Options for Scoliosis
If you suspect your child may have scoliosis, a consultation with a medical professional is an important next step toward an accurate diagnosis and an appropriate management plan. This process helps determine the severity of the condition and identify the most suitable scoliosis treatment approach.
The Diagnostic Process
- Clinical examination: The clinician will take a family and medical history, visually assess for asymmetry, and perform the Adam’s Forward Bend Test.
- X-ray imaging: This is the gold standard for diagnosing scoliosis. A full-spine X-ray allows the clinician to accurately measure the Cobb angle, which both confirms the diagnosis and provides a baseline for monitoring how the curve progresses over time.
- Ongoing monitoring: The frequency of follow-up appointments and X-rays will depend on your child’s age and the degree of curvature. Children in periods of rapid growth are typically reviewed every 4 to 6 months.
Treatment Options
Treatment is individualised based on three key factors: your child’s age and remaining growth potential, the severity of the curve (Cobb angle), and the type of scoliosis present.
- Observation and Monitoring (Cobb angle < 25°): For mild curves in children who are still growing, a “watch and wait” approach is generally recommended. Regular reviews are scheduled to monitor whether the curve progresses. During this period, physiotherapy for scoliosis and targeted exercises play an important role in strengthening the back and abdominal muscles, improving posture, and potentially helping to slow curve progression.
- Spinal Bracing (Cobb angle 25°– 40°): For children with significant remaining growth potential and a moderate curve, spinal bracing is often the preferred approach. Goal: The primary aim of wearing a back brace for scoliosis is to prevent the curve from worsening — not to fully straighten the spine. How it works: A TLSO (Thoracic-Lumbar-Sacral Orthosis) brace is custom-fitted to apply corrective pressure at key points along the curve, helping to hold the spine in a more upright position. Compliance: For bracing to be effective, it needs to be worn for 16 to 23 hours per day. The cooperation of both the child and the family is essential to the success of this approach.
- Spinal Surgery (Cobb angle > 45°– 50°): Surgical intervention is typically considered when the curve is severe, progressing rapidly despite bracing, or beginning to affect respiratory or cardiovascular function. Goal: Surgery aims to significantly correct the curvature and stabilise the spine in its new position using metal rods and screws. This can improve body balance, reduce the risk of serious complications, and improve posture. The decision to proceed with surgery is always carefully weighed against potential risks and benefits, in close discussion with the family.


A collaborative, multidisciplinary approach — involving paediatricians, orthopaedic specialists, physiotherapists, and psychologists where needed — forms the foundation of a comprehensive and successful management plan for your child.
Prevention and Effective Management of Scoliosis
While idiopathic scoliosis cannot be entirely prevented given its likely genetic component, building good habits and detecting the condition early can help reduce the risk of significant progression and support a better quality of life for your child.
Early Intervention and Building Healthy Habits
- Regular screening: Proactively check your child’s back from around age 10 and throughout adolescence — especially if your child is female or has a family history of scoliosis.
- Teaching good posture habits:
- When studying: Ensure the desk and chair are at the right height, so your child can sit with a straight back and feet flat on the floor. Encourage them to stand up and move around every 30 to 45 minutes.
- When standing: Encourage an upright posture with relaxed, level shoulders — avoiding the habit of leaning all body weight onto one leg.
- Using a backpack correctly:
- Avoid overloading the bag — aim to keep it within 10–15% of your child’s body weight.
- Always wear both straps to distribute weight evenly across both shoulders. While carrying a bag on one shoulder is not a direct cause of idiopathic scoliosis, it can contribute to poor postural habits and place additional strain on the spine.
- Be aware of flat feet and their connection to posture: Flat feet can alter the body’s alignment, creating a compensatory chain reaction that travels upward — affecting the knees, hips, and spine. If your child has flat feet, a clinical assessment may be worthwhile to explore whether orthopaedic insoles could help improve overall postural alignment.
The Risks of Flat Feet: Signs, Identification, and Effective Treatment
Day-to-Day Management for a Better Quality of Life
For children already diagnosed with scoliosis, supporting their management at home alongside medical treatment is an important part of the overall plan.
- Guided exercise for scoliosis: Specialised physiotherapy approaches — such as the Schroth method — are designed to strengthen weakened muscle groups, stretch muscles that have become tight, and teach children how to breathe more effectively to support lung capacity.
- Encouraging suitable physical activity: Symmetrical, low-impact activities such as swimming, walking, gentle cycling, and yoga are generally well-suited for maintaining flexibility and muscle strength without placing excessive load on the spine.
- Emotional and psychological support: Adolescence is a sensitive time. Having to wear a brace or feeling self-conscious about appearance can affect a young person’s confidence and self-esteem. Parents play an invaluable role as a source of encouragement, active listening, and steady support through these challenges.
Closing Thoughts
Scoliosis in children is a relatively common condition that can often be well-managed with timely attention and appropriate care. From recognising the earliest signs of asymmetry to following through on a clinician-recommended plan — whether that involves monitoring, physiotherapy, bracing, or surgery — each step contributes meaningfully to your child’s long-term health and wellbeing.
Parents are often the first to notice something is different. By checking regularly and seeking assessment as soon as you have concerns, you are giving your child the best opportunity for early, effective intervention — helping to prevent complications and supporting their confidence as they grow.
Don’t hesitate to reach out to Maple Healthcare – Chiropractic & Wellness Center for guidance and early support whenever you need it.
FAQ: Common Questions About Scoliosis in Children
Can scoliosis in children resolve on its own?
Answer: In most cases, idiopathic scoliosis does not resolve on its own and tends to progress during periods of growth. This is why ongoing monitoring and appropriate medical management, as guided by a clinician, are important.
Can carrying a heavy backpack cause scoliosis?
Answer: Carrying a heavy or one-sided bag is not considered a primary cause of idiopathic scoliosis. However, it can worsen postural imbalance and contribute to back pain. Encouraging good posture habits in children — including wearing a backpack correctly with both straps — is a sensible step in supporting spinal health.
What sports are appropriate for a child with scoliosis?
Answer: Symmetrical, low-impact activities such as swimming, walking, cycling, and yoga are generally encouraged. That said, before starting or continuing any exercise programme for scoliosis, it is best to consult your child’s clinician or physiotherapist to receive advice tailored to their specific condition and curve.
Related articles:
Contact for consultation
MAPLE INTERNATIONAL CO., LTD
Phone: 0705 100 100
Tax code: 0311948301
Date Range: 21 - 08 - 2012
Issued: Department of Planning and Investment of Ho Chi Minh City
Healthcare Group Members

Contact Us
COPYRIGHT

![]()