Golfer's Elbow: Causes, Symptoms And Treatment Guide
That nagging pain on the inner side of your elbow when gripping, rotating your wrist, or even typing may not be just an ordinary ache. It could be a sign of medial epicondylitis, more commonly known as golfer’s elbow. Despite the name, this condition is surprisingly common among office workers, gym-goers, and people whose jobs involve repetitive hand movements.
Medial epicondylitis (Golfer’s Elbow) is a musculoskeletal condition caused by damage or irritation at the point where the wrist flexor and forearm pronator tendons attach to the medial epicondyle of the humerus. According to medical literature, it is classified as a tendon overload disorder that can result from repeated micro-trauma.
This article aims to give you a comprehensive and easy-to-understand overview to help you:
- Recognise early symptoms so you can seek timely care.
- Understand the underlying causes so you can adjust your lifestyle and work habits.
- Learn about effective conservative treatment options and rehabilitation exercises.
- Know when it is time to seek professional medical advice and what recovery may look like.
Please note: The information in this article is intended for general reference only and is not a substitute for diagnosis or personalised advice from a qualified specialist.
What Is Medial Epicondylitis?
To better understand this condition, let us take a brief look at the anatomy and mechanism behind it.
Basic Anatomy of the Elbow
- Medial epicondyle: This is the bony bump you can feel on the inner side of your elbow.
- Tendon attachment point: The medial epicondyle serves as the common attachment point for a group of tendons, most notably the wrist and finger flexor tendons and the pronator teres muscle (which helps rotate the forearm palm-down).
- Function: These muscles and tendons are responsible for movements such as bending the wrist (curling the palm toward the forearm), gripping with the fingers, and rotating the forearm inward (pronation).
How It Develops: More Than Just “Inflammation”
When you repeatedly perform wrist flexion or forearm pronation movements under high load, the tendons at their attachment to the medial epicondyle are placed under excessive strain. Over time, this leads to micro-trauma.
Your body attempts to repair these small injuries, but if overloading continues, the healing process becomes disrupted. The result is tendon degeneration, where the collagen fibres become disorganised, the tendon may thicken, and small tears can form. Modern medical literature therefore tends to classify this condition as a tendinopathy rather than a straightforward inflammatory process.
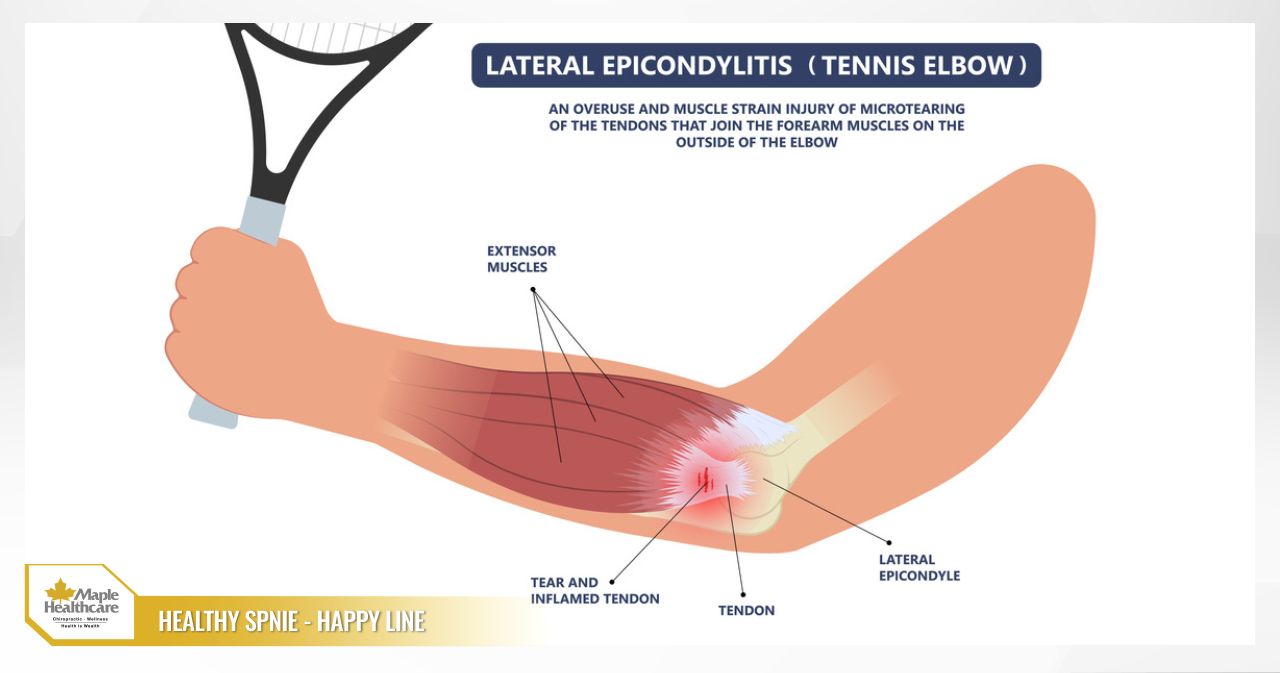
How to Tell It Apart from Tennis Elbow (Lateral Epicondylitis)
Many people confuse golfer’s elbow with tennis elbow. Here is a quick comparison of the two conditions:
Medial Epicondylitis (Golfer’s Elbow)
- Location of pain: Inner side of the elbow.
- Tendons involved: Wrist flexor tendons and forearm pronator muscles.
- Movements that provoke pain: Wrist flexion, gripping, forearm pronation.
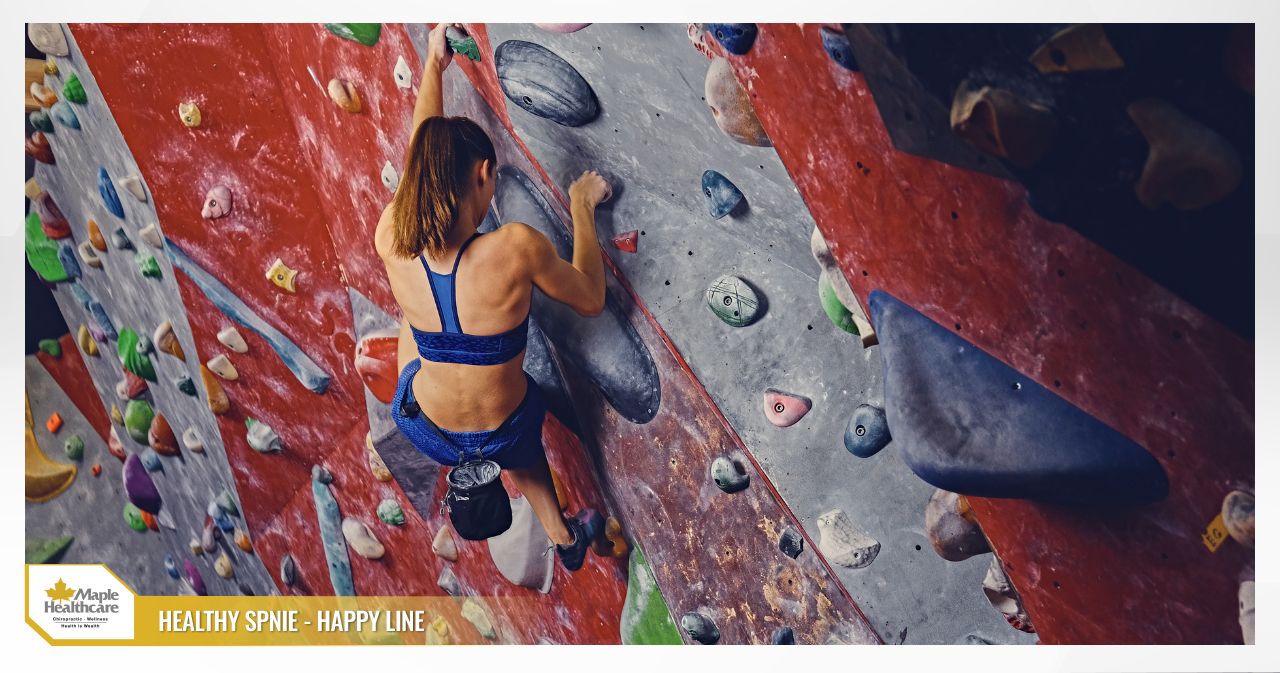
- Commonly associated sports: Golf, throwing sports, indoor rock climbing.
Lateral Epicondylitis (Tennis Elbow)
- Location of pain: Outer side of the elbow.
- Tendons involved: Wrist extensor tendons.
- Movements that provoke pain: Wrist extension, forearm supination, lifting objects.
- Commonly associated sports: Tennis, badminton, rowing.

Common Signs and Symptoms of Golfer’s Elbow
The symptoms of golfer’s elbow tend to develop gradually and may worsen if left unaddressed. Common signs include:
- Pain on the inner side of the elbow: This is the hallmark symptom. The pain is typically localised to the medial epicondyle and is often tender to the touch. It tends to worsen with activities such as: gripping tightly (handshakes, holding weights), bending the wrist against resistance (carrying heavy bags), and twisting the forearm (using a screwdriver, turning a door handle).
- Stiffness and weakness: You may notice stiffness in the elbow, particularly in the morning. Grip strength may feel reduced, making it difficult to hold objects securely or causing you to drop things.
- Reduced forearm endurance: The forearm may tire more quickly than usual during repetitive tasks such as typing, using a mouse, or exercising.
- Numbness or tingling (a warning sign): In some cases, swelling and irritation can affect the ulnar nerve, which runs nearby. This may produce a sensation of numbness, tingling, or pins and needles radiating down the inner forearm toward the ring finger and little finger.
The pain may range from acute (lasting days to weeks after overexertion) to chronic (persisting for more than three months, recurring repeatedly).
Causes and Risk Factors
The primary cause is repetitive overloading of the wrist flexor and forearm pronator tendons. Risk factors can stem from sports, work, and individual health characteristics.
- Sports and physical activity: Golf (poor swing mechanics), throwing sports (baseball), tennis (topspin shots), gym training (barbell curls, pulling exercises with poor grip technique), and indoor rock climbing.
- Occupational and daily activities: Carpenters, plumbers, and construction workers who frequently use hammers or wrenches. Office workers who spend extended hours at a keyboard and mouse with poor wrist posture.
- Poor technique and training habits: Sudden increases in training volume or intensity. Insufficient warm-up before activity and inadequate rest days.
- Poorly fitted equipment: Golf clubs or tennis rackets that are the wrong grip size. Work tools with handles that do not fit the hand well. A poorly sized computer mouse.
- Individual health factors: Age (most commonly seen in people aged 35–55), obesity, smoking, and pre-existing conditions such as diabetes or rheumatoid arthritis.
When Should You See a Doctor?
If your symptoms are mild and have only just appeared, self-care at home may be appropriate. However, please seek assessment from a musculoskeletal or rehabilitation specialist if you notice any of the following:
- Pain has lasted more than 2–3 weeks without improvement despite rest.
- Pain is worsening, present at rest, or waking you at night.
- Noticeable weakness in your grip, difficulty performing daily tasks, or frequently dropping objects.
- Signs of ulnar nerve involvement: spreading numbness or loss of sensation in the little finger and ring finger.
- Swelling, warmth, redness, or visible deformity at the elbow.
- Pain began after an acute injury, with concern about a tendon tear or ulnar collateral ligament (UCL) damage.
- You have tried self-care consistently for 4–6 weeks without meaningful improvement.
How Is Golfer’s Elbow Diagnosed?
Diagnosis of golfer’s elbow is primarily based on a detailed medical history and clinical examination. Imaging investigations are only used when other causes need to be ruled out or when the diagnosis is unclear.
- Medical history: Your doctor will ask in detail about your occupation, sporting habits, when the pain started, what makes it better or worse, and any history of injury.
- Clinical examination: Your doctor will perform specific tests to pinpoint the exact location and cause of pain, such as pressing on the medial epicondyle, asking you to flex your wrist against resistance, and screening for any ulnar nerve involvement.
- Investigations (when needed):
- Ultrasound: A useful tool for directly assessing the tendon, detecting thickening, degeneration, or small tears.
- X-ray: Ordered to rule out bony problems such as bone spurs, calcification, or joint arthritis.
- MRI (Magnetic Resonance Imaging): Used in complex cases where associated injuries are suspected, such as significant tendon tears or ligament damage.
- Functional assessment tools: Your doctor may use questionnaires such as the QuickDASH to measure how much the pain is affecting your arm function and to monitor your progress through treatment.

Conservative Treatment: The First Line of Care for Golfer’s Elbow
The encouraging news is that more than 90% of golfer’s elbow cases respond well to conservative management. The key principles are reducing load on the tendon, managing pain, and then systematically rebuilding tendon strength.
- Relative rest: Avoid activities that provoke sharp pain, while maintaining gentle movement within a comfortable range to prevent stiffness.
- Ice and heat: Apply ice during the acute phase; use warmth during the chronic phase before exercise.
- Medication as directed by your doctor: Non-steroidal anti-inflammatory drugs (NSAIDs) in oral or topical gel form may be prescribed for short-term use.
- Bracing or strapping: A counterforce brace around the forearm may help reduce strain on the tendon during activity, but should not be relied upon as a long-term solution.
- Physiotherapy and rehabilitation: This is the cornerstone of treatment and includes hands-on therapy, pain relief modalities (therapeutic ultrasound, TENS), extracorporeal shockwave therapy (ESWT), and ergonomics education.
At Maple Healthcare in Ho Chi Minh City, clinicians and physiotherapists work together to develop a personalised conservative treatment plan that combines these approaches. The goal is to support pain reduction, restore movement, and help reduce the risk of recurrence in a safe, structured way.
Rehabilitation Exercises
Exercise is the most important element for rebuilding the tendon’s capacity to handle load. Move gently and listen to your body throughout.
Warm-Up (2–3 Minutes)
- Gently rotate your wrist and elbow joints.
- Open and close your hand in a slow, rhythmic manner.
Stretching (Hold 20–30 Seconds, Repeat 3–5 Times, Twice Daily)
Wrist flexor stretch: Extend your arm straight in front of you with your palm facing upward. Use your other hand to gently pull your fingers and hand downward until you feel a mild stretch along the inner forearm.
Isometric Strengthening (Early Stage, When Pain Is Significant)
Isometric wrist flexion: Rest your forearm on a table with your palm facing upward. Place your other hand on top of the palm of the affected side. Contract your muscles as if trying to bend your wrist upward, while your other hand resists the movement so no motion occurs. Hold for 5–10 seconds and repeat 10 times.
Eccentric Strengthening (Later Stage, Once Pain Has Settled)
Eccentric Wrist Flexion: Hold a light weight (a small water bottle or 0.5 kg dumbbell). Rest your forearm on a table with your palm facing upward. Use your unaffected hand to lift the affected wrist into a fully flexed position. Then release the unaffected hand and slowly lower the wrist back down in a controlled manner over 3–5 seconds. Repeat for 3 sets of 12–15 repetitions.
Shoulder, Scapular, and Core Stability
Weakness in the shoulder and core kinetic chain can place greater stress on the elbow. Exercises such as planks, rotator cuff strengthening, and scapular stability work help build a solid foundation and reduce the overall load on the arm.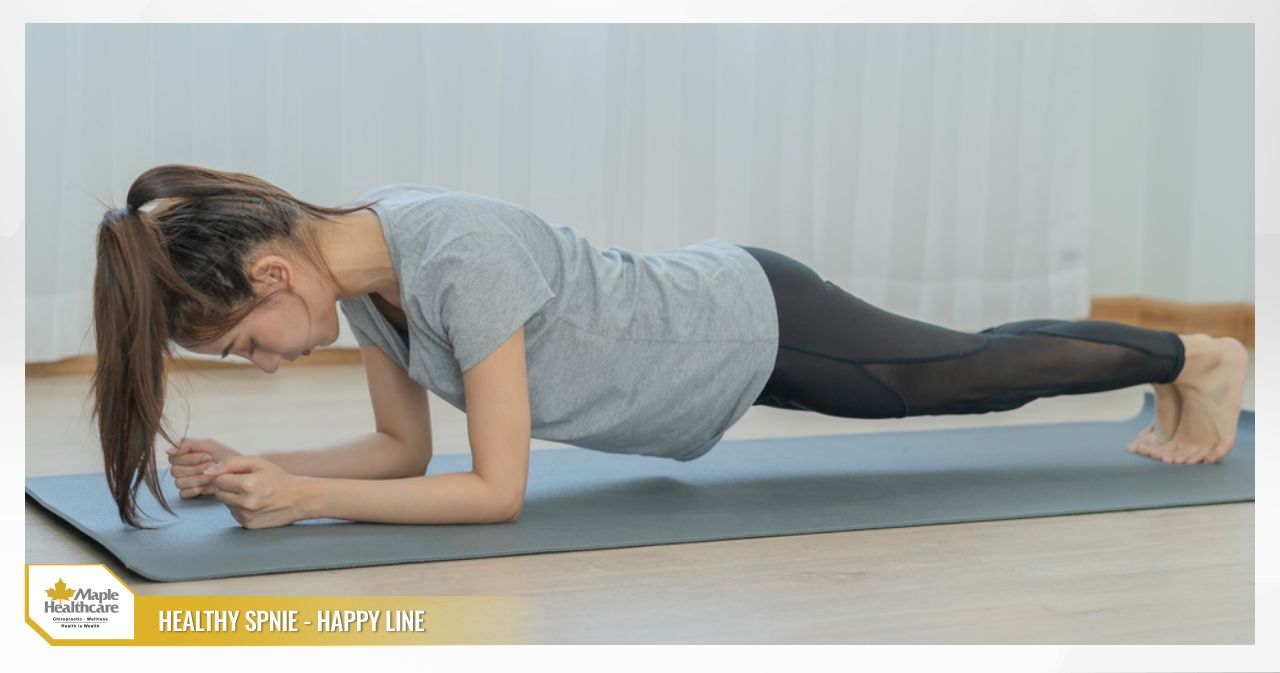
Injection and Procedural Options
When conservative treatment has not produced adequate results over time, your doctor may consider the following options:
- Corticosteroid injection: This can provide meaningful short-term pain relief, but carries a risk of tendon weakening or rupture if used too frequently.
- Platelet-Rich Plasma (PRP): This uses your own blood to stimulate the body’s natural healing response. Evidence on its effectiveness is still being evaluated through ongoing research.
Surgery for Golfer’s Elbow
Surgery is considered a last resort and is appropriate for only a small proportion of patients (fewer than 10%) — those for whom intensive conservative management over at least 6–12 months has not been effective, whose pain is severe, or who have significant structural damage. The surgical approach typically involves removing the affected tendon tissue and repairing the remaining tendon.
Preventing Golfer’s Elbow
You can meaningfully reduce your risk of developing or experiencing a recurrence of golfer’s elbow with the following measures:
- Refine your technique: Work with a qualified coach to ensure proper form in your sport or activity.
- Progress gradually: Follow the principle of increasing training volume, intensity, or duration by no more than 10% per week.
- Warm up and cool down: Always warm up before sport or heavy work, and stretch adequately afterwards.
- Use well-fitted equipment: Make sure your clubs, rackets, and work tools are the right size and weight for your hand.
- Optimise your workstation ergonomics: Adjust your chair and desk height, use an ergonomic mouse and keyboard, and take short breaks every 30–45 minutes.
Recovery Timeline and Outlook
Recovery time for golfer’s elbow depends on the severity of the injury and how consistently you follow your treatment plan:
- Mild to moderate cases: When caught early and managed consistently, most people notice meaningful improvement within 6 to 12 weeks.
- Chronic cases: These may take 3 to 6 months, or sometimes longer, to reach full recovery. Patience and consistency are key to a successful outcome.
FAQ: Common Questions About Golfer’s Elbow
Can golfer’s elbow heal on its own?
Answer: Very mild cases may improve with timely rest and load reduction. However, most cases benefit from a structured rehabilitation programme to avoid the condition becoming chronic or recurring.
Should I use ice or heat?
Answer: During the acute phase (recent onset, swelling present), ice is generally recommended. During the chronic phase (persistent dull ache, stiffness), you may apply warmth before exercise and ice afterwards if discomfort arises.
Should I wear an elbow brace?
Answer: A counterforce brace can help manage pain during the acute phase, but it is not a long-term solution. It works best when combined with a strengthening programme aimed at building lasting tendon resilience.
When would I need an MRI?
Answer: Your doctor may recommend an MRI if there is concern about a tendon tear, ligament injury, ulnar nerve compression, or if your symptoms have not responded to standard conservative treatment.
Do I need to stop going to the gym completely?
Answer: Not necessarily. It is generally advisable to temporarily avoid exercises that directly provoke pain (such as barbell curls) and shift your focus to other muscle groups, such as legs and core. A physiotherapist can help you modify your training programme so you can stay active safely while your elbow recovers.
Related articles:
Contact for consultation
MAPLE INTERNATIONAL CO., LTD
Phone: 0705 100 100
Tax code: 0311948301
Date Range: 21 - 08 - 2012
Issued: Department of Planning and Investment of Ho Chi Minh City
Healthcare Group Members

Contact Us
COPYRIGHT

![]()